Ijikc.co.in
ISSN: 2454-2415
Volume 2, Issue 1, January, 2016
International Journal of
Innovative Knowledge
Concepts
Premenstrual Symptoms and Social Disability
Nabhit Kapur1 and Prabhjeet Singh Narula2
1Director ,Peacfulmind training center
Asst Coordinator, Peacfulmind Training Center
Abstract :
Background: A woman menstruation is believed to be suffering from premenstrual syndrome
(PMS) when she experiences recurring physical and/or psychological symptoms occurring
specifically during the luteal phase of the menstrual cycle and that often resolve by the end of the
cycle (O'Brien, 1987)
.
Up to 75% of women experience some degree of premenstrual syndrome (PMS) during their reproductive years. Somatic symptoms, such as fatigue, appetite-changes, and low energy, and affective symptoms, such as irritability, depressed mood, anxiety, and impulsive behaviour constitute this condition. Impairment difficulties such as physical functioning, psychological health and severe dysfunction in social or occupational realms are believed to be possible causes of premenstrual symptoms. Poor health related quality of life in women with PMS and its negative effect on school functions and social interactions in young adolescents has been shown in some previous studies (Delara, Ghofranipour, Azadfallah, Tavafian, Kazemnejad, & Montazeri, 2012).
Purpose: The main objective of this study is to examine the impact of premenstrual
symptoms on social adjustment.
Material And Methods: Around 40 randomly selected, healthy females, aged between 18-45 yrs.;
experiencing regular menstrual cycle were administered the two questionnaires, ‗The
Premenstrual Symptoms Screening tool (PSST)‘ and ‗Sheehan Disability Scale (SDS)‘, analyzing
their degree of premenstrual symptoms and the effect of premenstrual syndrome on their daily life
activities. Pearson product-moment correlation coefficient method has been used to analyse the
relationship between premenstrual symptoms and its impact on social adjustment.
Results: As per the average score obtained through premenstrual symptoms screening tool
(PMSST), 16 (40%) of the women undergoing the survey were found to be suffering from mild
form of premenstrual syndrome and interestingly 10 (25%) and 7 (18%) out of the total number of
women (40) surveyed were having moderate and severe premenstrual syndrome respectively.
Analysis of Sheehan Disability Scale revealed that out of 40 women surveyed, 19 (48%), 20 (50%) and 17 (43%) women experienced mild disruption in their work, social life and family life respectively accounting to the premenstrual symptoms. Likewise, moderately disrupted work, social life and family life was found to be experienced by 11 (28%), 13 (33%) and 15 (38%) respectively out of the total number of women being surveyed
It was also evident from the responses of Sheehan Disability Scale that 58% of the women being surveyed had reduced productivity at work due to premenstrual symptoms.
A significantly positive correlation between premenstrual syndrome and social disability was also noted by analysis of the data, which implies that when premenstrual symptoms and/or their severity increases, the chances of social disability increases & vice versa
Conclusion: Most of the women experienced difficulties in their daily work, social life as well as
family life to a certain extent pertaining to mild to moderate premenstrual symptoms. Moreover,
with increase in severity of the premenstrual symptoms, the productivity at work also tends to
decrease thereby indicating a positive correlation between premenstrual symptoms and social
disability.
Keywords: Premenstrual Symptoms, Social Disability
Available online at www.ijikc.co.in
Premenstrual Symptoms and Social Disability.
1 INTRODUCTION:
headache, bloating, sleep disturbances, appetite change, poor concentration, decreased interest,
A woman experiencing recurring physical
social withdrawal, irritability, mood swings,
anxiety/tension, depression, and feeling out of
specifically during the luteal phase of the menstrual
cycle and often resolving by the end of
Tavafian, Kazemnejad, & Montazeri, 2012).
menstruation is believed to be suffering from
Premenstrual tension was first defined in 1930s,
premenstrual syndrome (PMS) (O'Brien, 1987). In
when women entered the workforce. It is stated that
particular, emotional symptoms must be present
women who had never worked outside the home
consistently to diagnose PMS. The specific
were less likely to report PMS (Namavar Jahromi,
emotional and physical symptoms attributable to
Pakmehr, & Hagh‐Shenas, 2011).
PMS vary from woman to woman, but each individual woman's pattern of symptoms is
Premenstrual symptoms might cause
predictable, occurs consistently during the ten days
prior to menses, and vanishes either shortly before
impairment in physical functioning, psychological
or shortly after the start of menstrual flow.
health and severe dysfunction in social or occupational
The definition of severe PMS varies
among Randomized controlled trials, however in
functions and social interactions in a negative way.
recent studies standardized criteria have been used
Previous studies have also shown that women with
to diagnose one variant of severe PMS —
premenstrual disorders have a poor health‐related
premenstrual dysphoric disorder. This criterion is
quality of life (Delara, Ghofranipour, Azadfallah,
based on at least five symptoms, including one of
Tavafian, Kazemnejad, & Montazeri, 2012).
four core psychological symptoms (from a list of 17 physical and psychological symptoms), being
Various risk factors include high caffeine
severe before menstruation starts and mild or
intake (Kaleli, 2001), Stress may precipitate
absent after menstruation (Steiner, Romano, &
condition, Increasing age, history of depression,
Babcock, 2001) (Freeman, Rickels, & Yonkers,
family history, dietary factors (Low levels of
2001). The 17 symptoms are depression, feeling
hopeless or guilty, anxiety/tension, mood swings,
magnesium, Vitamin B‐6 (Wyatt, Paul, Peter, & P
irritability/persistent anger, decreased interest, poor
M Shaughn, 1999), manganese, zinc (Chuong &
concentration, fatigue, food craving or increased
Dawson, 1994), vitamin E and also Vitamin D).
appetite, sleep disturbance, feeling out of control or
PMS is generally a stable diagnosis, with
overwhelmed, poor coordination, headache, aches,
swelling/bloating/weight gain, cramps, and breast
symptoms at the same intensity near the end of
each cycle for years. Treatment for specific
symptoms is usually effective at controlling the
syndrome experience only a few of the possible
symptoms. Even without treatment, symptoms tend
symptoms, in a relatively predictable pattern. For
to decrease in perimenopausal women, and
example, one woman with PMS may be anxious
disappear at menopause (Roca, Schmidt, &
and tense for three or four days before her
menstrual period begins, and this will happen with
In a comprehensive review of the
only small variations each cycle, such as being
literature Parkin and Winer distinguished four
somewhat more tense (or less tense) than in
types of studies that evaluated the PMS/PMDD
previous cycles (Yonkers, 2008).
effect on health‐related quality of life and for
Up to 75% of women experience some
instance reported that ‗the affective, behavioral and
degree of premenstrual syndrome (PMS) during
physical symptoms of PMDD have been shown to
their reproductive years. This condition includes
adversely affect health‐related quality of life to a
somatic symptoms, such as fatigue, appetite‐
disabling degree, especially regarding interpersonal
changes, and low energy, and affective symptoms,
relationships with family members and partner‘ or
such as irritability, depressed mood, anxiety, and
‗women with PMDD suffer impairment that is as
impulsive behavior. Typically, symptoms remit
severe as women with chronic clinical depression
within a few days after the onset of menstruation
and that their luteal phase adjustment to social and
(Hoyer, et al., 2013).
leisure activities is even worse than women with other types of depression‘ (Pearlstein & Steiner,
Premenstrual symptoms represent an
affective syndrome the appearance of which is confined to the luteal phase of the menstrual cycle
2 REVIEW OF LITERATURE:
and the symptoms of which are sufficiently severe to interfere with normal life activities (Rubinow &
Numerous studies indicate that work stress
Schmidt, 2006). The common symptoms of PMS
may exacerbate PMS. In a recently conducted
survey study in Uppsala County, Sweden, 83
International Journal of Innovative Knowledge Concepts
, 2(1) January, 2016
Premenstrual Symptoms and Social Disability.
women stated that they had been absent from work
and mental health (MH) scales and greater than
during the previous half year due to premenstrual
type 2 diabetes and hypertension in bodily pain
discomfort (premenstrual syndrome, PMS). The
scale while comparable in all other scales of the
absence due to illness and the diagnoses of these
three conditions, (2) comparable to osteoarthritis
women during an 1 year period were compared
and rheumatoid arthritis in all scales, and (3) less
with those of a control group which was matched in
burden than depression in vitality and mental health
terms of number of women, age and civil status,
(MH) scales and mental component summary
but in which the women did not report suffering
measure while comparable in other scales (Yang,
from PMS. The results show more illnesses and a
Wallenstein, Hagan, Guo, Chang, & Kornstein,
different diagnostic pattern when absent from work
(due to illness) in women suffering from PMS as
A cross‐sectional cohort study conducted
compared with the control group. The diagnosis ‗mental disorders‘ is twice as common in the group
in 2003 on women prospectively diagnosed with PMS revealed interesting findings such as, 28.7%
absent due to PMS (Hallman & Georgiev, 1987).
of the women amongst the total number of women
Studies have shown that Women under‐
completing the survey were found to be suffering
identify the severity of their PMS difficulties
from PMS. These women with PMS had
despite the reported difficulties associated with
consistent social and occupational interference in
Component Summary
(MCS) and Physical
most life domains. They are also reluctant to seek
Component Summary (PCS) scale scores of the
help for treatable PMS symptoms because of
Medical Outcomes Study Short Form‐36 as
attitudinal barriers regardless of the severity of
compared to women without PMS. Moreover,
their PMS symptoms (Robinson & Swindle, 2000).
women with PMS reported reduced work productivity, interference with hobbies and greater
Studies also suggest that in spite of the
number of work days missed for health reasons
high prevalence of PMS, this condition is still
along with an increased frequency of ambulatory
under‐recognized and undertreated. Using self‐help
health care provider visits as compared to the
approaches to induce self‐awareness, psychological
women without PMS. Conclusively the study
and psychiatric interventions, and appropriate
suggests that premenstrual symptoms significantly
medications may help susceptible women with high
affect health‐related quality of life and may result
work stress to overcome this cyclic condition in
in increased health care utilization and decreased
order to increase their productivity and quality of
occupational productivity (Borenstein, et al., 2003).
life (Namavar Jahromi, Pakmehr, & Hagh‐Shenas, 2011).
A cross‐sectional population‐based survey
conducted in 2010 on 4,085 women aged 14‐ 50
A recent study conducted on Korean
years recruited by random telephone digit dialing in
women revealed the impact of PMS on activities of
France, Germany, Hungary, Italy, Spain, the United
daily life and also suggested that the proportion of
Kingdom, Brazil, and Mexico also found that both
women with impaired activities of daily life were
physical and mental premenstrual symptoms had
significantly associated with the severity of PMS
significant impact on quality of life. Up to 35% of
(Choi, Lee, Lehert, Lee, Kim, & Dennerstein,
women of reproductive age in Europe and Latin
America were moderately or severely affected in
Similarly, another study conducted in
activities of daily life by cyclical premenstrual
cities of Hong Kong, Thailand and Pakistan
symptoms (Dennerstein, Lehert, Bäckström, &
demonstrated that premenstrual physical and
Heinemann, 2010).
mental symptom domains had similar negative
Likewise another study conducted in 2011
effects on activities of daily life in women. 74% of
with an aim to analyze the frequency of
women were not affected or minimally affected in
Premenstrual Syndrome (PMS) in college students,
activities of daily life, 17% had a clinically
the factors affecting Premenstrual Syndrome and
significant effect on activities of daily life and 9%
the effect of Premenstrual Syndrome on life quality
were severely affected in activities of daily life.
found that among 316 students PMS was detected
Activities of daily life were predominantly affected
in 72.1% of the students. The most frequent
by premenstrual symptom severity (Dennerstein,
symptoms were mainly low back pain, stress‐
Lehert, Keung, Pal, & Choi, 2010).
discomfort, nervous‐anger, distention and breast
Likewise, a study on assessment of burden
tenderness. PMS was found significantly high in
of premenstrual dysphoric disorder on health‐
those students who had menstrual irregularity, who
related quality of life found that premenstrual
had dysmenorrhea, who consumed 2 cups of coffee
dysphoric disorder is associated with substantial
or above per day and who smoke and consumed
burden on both physical and mental aspects of
alcohol. When the relation of PMS with life quality
health related quality of life. The findings of the
was evaluated, it was determined that the life
study were that the health related quality of life
quality decreases as PMS score average increases
burden of premenstrual dysphoric disorder was (1)
(Pinar, Colak, & Oksuz, 2011).
greater than that of chronic back pain in bodily pain
International Journal of Innovative Knowledge Concepts
, 2(1) January, 2016
Premenstrual Symptoms and Social Disability.
SIGNIFICANCE OF STUDY:
and social impairment.
Numerous studies indicate that work stress
2. To examine the effect of PMS on
may exacerbate PMS. Women have been found to
work/school life.
be absent from work during the previous half year
3. To examine the effect of PMS on social
due to premenstrual discomfort (premenstrual
syndrome, PMS). The results of studies have revealed more illnesses and a different diagnostic
4. To examine the effect of PMS on family
pattern when absent from work (due to illness) in
women suffering from PMS as compared with the
5 HYPOTHESIS:
control group. Moreover it was also found that the group of women absent from work due to PMS had
There is a statistically significant inverse
the diagnosis ‗mental disorders‘ twice as common
relationship between premenstrual symptoms and
as compared to the control group (Hallman &
social disability.
Georgiev, 1987). Moreover, Women under‐identify the severity of their PMS difficulties despite the
6 RESEARCH METHODOLOGY:
reported difficulties associated with consistent
6.1 SAMPLE
social and occupational interference in most life domains. They are also reluctant to seek help for
Around 40 randomly selected, healthy
treatable PMS symptoms because of attitudinal
females, aged between 18‐45 yrs.; experiencing
barriers regardless of the severity of their PMS
regular menstrual cycle were administered the two
symptoms (Robinson & Swindle, 2000).
premenstrual symptoms and another questionnaire
A recent study conducted on Korean
analyzing the effect of premenstrual syndrome on
women revealed the impact of PMS on activities of
their daily life activities.
daily life and also suggested that the proportion of women with impaired activities of daily life were
6.2 TOOLS
significantly associated with the severity of PMS
In order to conduct the study, following tools were
i.e. with increasing severity of the symptoms of
PMS the activities of daily life of such women decreased significantly (Choi, Lee, Lehert, Lee,
1.
‘The Premenstrual Symptoms Screening
tool (PSST)'
Kim, & Dennerstein, 2010).
(Appendix I): PSST applies a
necessary degree of measure of severity and
Similarly, another study conducted in
impact of premenstrual symptoms. The
Europe and Latin America, it was found that up to
questionnaire comprises of 13 questions which
35% of women of reproductive age were
are basically symptoms of premenstrual phase
moderately or severely affected in activities of
and the subjects are required to mark the
daily life by cyclical premenstrual symptoms
severity of each symptom as they had
(Dennerstein, Lehert, Bäckström, & Heinemann,
experienced in a scale of 1 to 5.
2.
‘Sheehan Disability Scale (SDS)' (Appendix
Likewise, study carried out on college students in
II): Developed to assess the functional
Turkey also found that the PMS rate was high even
impairment in three inter‐related domains;
in female college students and this adversely
work/school, social and family life. The
affected their quality of life and daily activities
subject rates the extent to which work/school,
(Pinar, Colak, & Oksuz, 2011).
social life and home
In spite of the high prevalence as
responsibilities are impaired by his/ her
suggested by the earlier studies, PMS is still under‐
symptoms on a 10 point visual analogue scale.
recognized and undertreated. Using self‐help
The 10 point visual analogue scale uses a
approaches to induce self‐awareness, psychological
spatiovisual, numeric and verbal descriptive
and psychiatric interventions and appropriate
anchors simultaneously to assess the disability.
medications may help susceptible women with high
The Sheehan Disability Scale is widely used
work stress to overcome this cyclic condition in
not only in psychiatry but also in many other
order to increase their productivity and quality of
chronic medical illnesses because of its generic
life (Namavar Jahromi, Pakmehr, & Hagh‐Shenas,
design. It measures impairment in functioning.
The scale generates 4 scores: a work disability score, a social life disability score, a family life
4 OBJECTIVES:
disability score and a total score. To get a total
The main objective of this study is to
score add up the 3 individual scores (work:
examine the impact of premenstrual symptoms on
social life: family life). The maximum possible
social adjustment. The specific objectives of the
score is 30 (Harnett‐Sheehan & Sheehan,
1. To examine the relationship between PMS
International Journal of Innovative Knowledge Concepts
, 2(1) January, 2016
Premenstrual Symptoms and Social Disability.
STATISTICAL ANALYSIS
regarding the symptoms of premenstrual syndrome (Appendix III) and the extent to
To analyze the data, Pearson product‐
which they experience them and the extent to
moment correlation coefficient method
which such symptoms affected their work,
social life and family life (Appendix IV) and
7 RESULT AND DISCUSSION:
final data of these 40 subjects [age range 22 – 43 yrs (Figure 1); mean age 29 years] was
A total of 40 subjects were surveyed
Table 1: Mean Age Of All 40 Subjects Enrolled And The Age Range
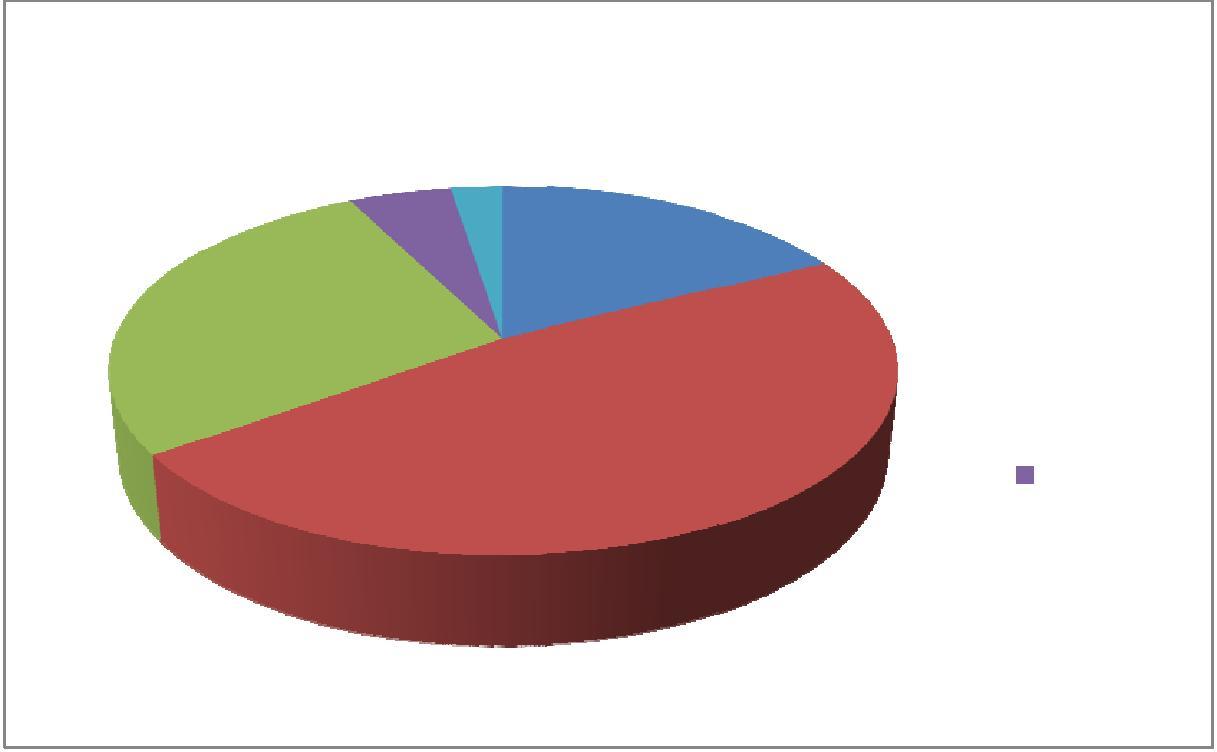
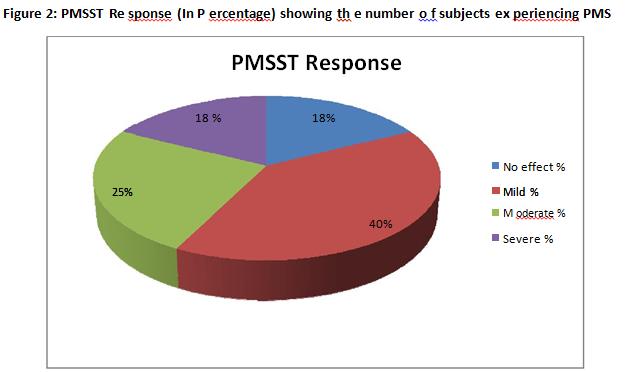
Out of 40 patients, as per the average score obtained through premenstrual symptoms screening tool
(PMSST) 7 (18%) of the women did not experience premenstrual symptoms while 16 (40%) of the women
undergoing the survey were found to be suffering from mild form of premenstrual syndrome and
interestingly 10 (25%) and 7 (18%) out of the total number of women surveyed were having moderate and
severe premenstrual syndrome respectively (Table 2, Figure 2).
Table 2: Average Score of PMSST showing the number of subjects experiencing the level of
symptoms
PMSST Response
Moderate PMS
Severe PMS
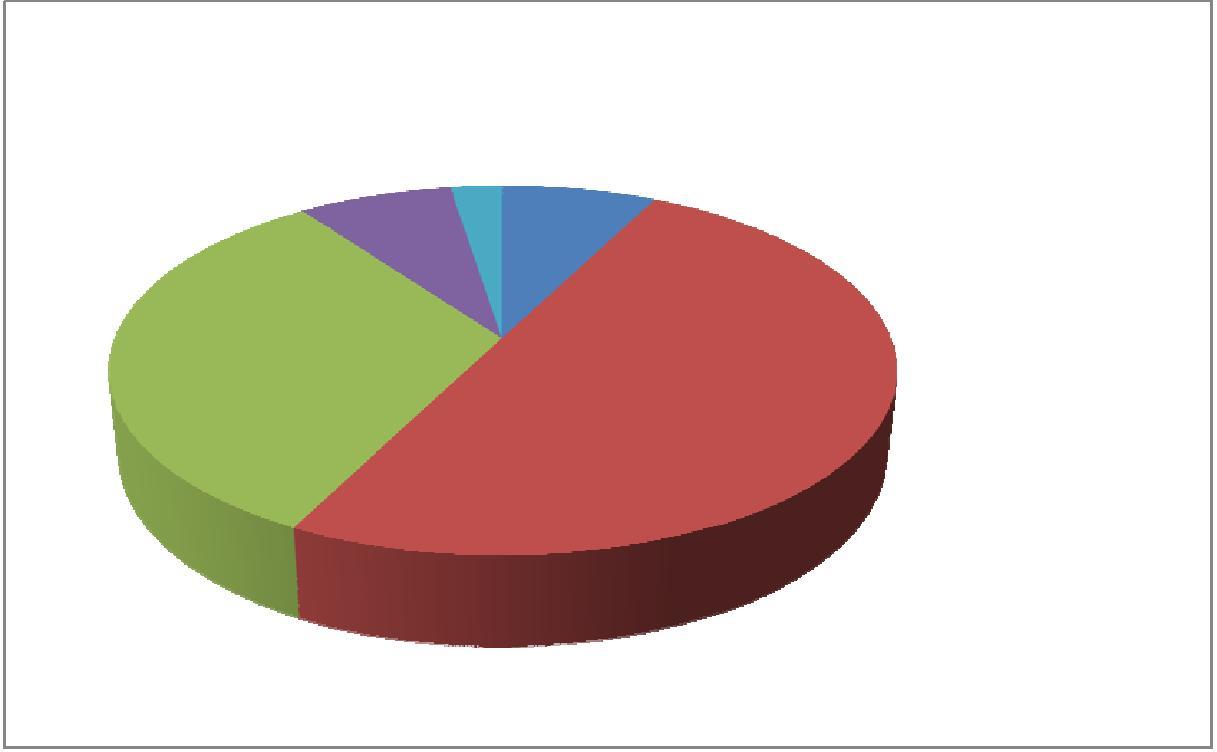
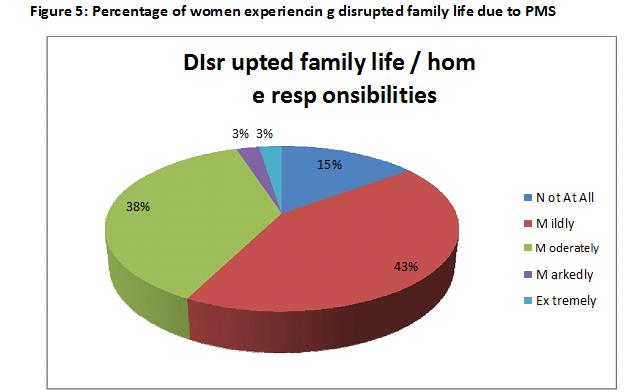
Moreover, analysis of Sheehan Disability Scale revealed that out of 40 women surveyed, 7 (18%), 3
(8%) and 6 (15%) of the women did not have a disrupted work, social life and family life respectively due to premenstrual symptoms. Whereas, 19 (48%), 20 (50%) and 17 (43%) women experienced mild disruption in their work, social life and family life respectively accounting to the premenstrual symptoms. Likewise, moderately disrupted work, social life and family life was found to be experienced by 11 (28%), 13 (33%) and 15 (38%) respectively out of the total number of women being surveyed. Similarly, 2 (5%), 3 (8%), 1 (3%) and 1 (3%), 1 (3%) , 1 (3%) women experienced markedly and extreme disruption respectively in their work, social and family life respectively (Table 3, Figure 3, Figure 4, Figure 5).
Data analysis of Sheehan Disability Scale also revealed Global Functional Impairment score, obtained
by summing up individual scores of disrupted work, disrupted social life and disrupted family life ranging from 0 (unimpaired) to 30 (highly impaired), to be interestingly 4 (10%), 14 (13%) and 29 (3%) out of the 40 women being surveyed (Table 4, Figure 6).
Furthermore, it was also evident from the responses of Sheehan Disability Scale that 23 out of 40 i.e.
58% of the women being surveyed had reduced productivity at work due to premenstrual symptoms.
International Journal of Innovative Knowledge Concepts
, 2(1) January, 2016
Premenstrual Symptoms and Social Disability.
Table 3: Number of women experiencing social disruption due to PMS
Not At All
Moderately
Markedly
Extremely
Disrupted
work / school
Disrupted
social life /
activities
DIsrupted
family life /
Table 4: Global Functional Impairment Score and Number of subjects
Global Functional
Number of
Impairment Score
Subjects
International Journal of Innovative Knowledge Concepts
, 2(1) January, 2016


Premenstrual Symptoms and Social Disability.
Figure 3: Percentage of women experiencin g disrupted work due to PMS
Disr upted work / school work
International Journal of Innovative Knowledge Concepts, 2(1) January, 2016
Premenstrual Symptoms and Social Disability.
Figure 4: Percentage of women experiencin g disrupted social life d ue to PMS
D isrupted social life / lei sure ac tivities
International Journal of Innovative Knowledge Concepts, 2(1) January, 2016
Premenstrual Symptoms and Social Disability.
Pearson‘s product correlation coefficient was used in order to find out the relationship between
premenstrual symptoms and social disability.
Social Disability
The value of R is 0.60. This is a moderate positive correlation, which means there is a tendency for
high X variable scores go with high Y variable scores (and vice versa).
If N is 10 or larger, the significance of calculating R will be tested by applying t‐ test. This test will
show the significance of the relationships.
The coefficient of correlation will vary from ‐ 1 (a perfect negative relationship between the
variables X & Y) to +1 (a perfect positive relationship between X and Y). If R comes to be closer to +1, it means there is a strong & positive correlation between the two variables & there is a complete association between the two variables whereas if R comes to be closer to ‐ 1, it means there is a strong negative correlation between the two variables. A correlation coefficient of 0 indicates no correlation between the variables.
The coefficient of Pearson correlation is 0.60 (The one‐ tailed P value is less than 0.0001). So, there
is a significantly positive correlation between premenstrual syndrome and social disability, which implies that when premenstrual symptoms and/or their severity increases, the chances of social disability increases & vice versa. Therefore, the hypothesis ―There is a statistically significant inverse relationship between premenstrual symptoms and social disability‖ is rejected.
This can be further analyzed in the light that when a person is undergoing or experiencing symptoms
like painful menstruation, insomnia, mood swings or irritability, headaches, bloating, fatigue etc., then a woman tends to become less productive in daily work and this also affects her daily work, social as well as family life to a certain extent. These findings are in consensus with earlier studies conducted on Korean women (Choi, Lee, Lehert, Lee, Kim, & Dennerstein, 2010) and a similar study conducted on students in Europe and Latin America (Dennerstein, Lehert, Bäckström, & Heinemann, 2010) as well as study conducted in Turkey (Pinar, Colak, & Oksuz, 2011), which suggest high prevalence of PMS and adversely affected quality of daily life and reduced productivity at work due to PMS.
The critical value of r at .005 level of significance & at 38 degrees of freedom is .4026 which is less
than calculated value of correlation coefficient, thus indicating that the relationship between PMS and social disability is significant even at 99.5% confidence.
8 Conclusion:
The findings of the study indicate that most of the women experience mild to moderate premenstrual
symptoms and this also affects their daily work, social life as well as family life to a certain extent. Moreover, with increase in severity of the premenstrual symptoms, the productivity at work also tends to decrease thereby
International Journal of Innovative Knowledge Concepts, 2(1) January, 2016
Premenstrual Symptoms and Social Disability.
indicating a positive correlation between premenstrual symptoms and social disability.
9 Limitations:
Limitations of the study include:
1) Small sample size due to time frame restriction
2) Lack of expertise with better statistical tools for analysis of data
3) Hesitant nature of women in responding to PMS questionnaire due to their belief that they were
not suffering from premenstrual symptoms which was in consensus with a recent study that found that PMS is still under‐ recognized and undertreated (Namavar Jahromi, Pakmehr, & Hagh‐Shenas, 2011)
10 Suggestions for further work:
The current study also suggests a positive correlation between PMS and social disability as other recent studies have suggested. However, similar study is required to be done at a larger scale as the current study had limited sample size due to logistic refrains. A larger scale study is also required to be done in order to gather more significant data to analyze correlation between PMS and social disability and also an attempt to analyze the precipitating factors. Moreover, no such study data could be found on Indian population thereby making it important to conduct such a study on Indian population also.
Furthermore, collecting such data will aid in creating better awareness strategies and creating educational methods which would help women identify premenstrual symptoms and aid in management of symptoms since the current study limitations has also shown that much of the women were not aware of premenstrual symptoms and although they were later on found to be suffering from PMS to some extent. Also, since it has been shown in various such studies including the current study that PMS also leads to decreased productivity at work, thus at least an awareness program and/or program to teach methods to manage the symptoms at gynaecology departments at hospitals as well as private clinics.
11 References:
Borenstein, J., Dean, B., Endicott, J., Wong, J., Brown, C., Dickerson, V., et al. (2003). Health and economic
impact of the premenstrual syndrome. J Reprod Med , 48 (7), 515‐ 524.
Choi, D., Lee, D. Y., Lehert, P., Lee, I. S., Kim, S., & Dennerstein, L. (2010). The impact of premenstrual
symptoms on activities of daily life in Korean women. Journal of Psychosomatic Obstetrics & Gynecology , 31 (1), 10‐ 15.
Chuong, C., & Dawson, E. (1994). Zinc and copper levels in premenstrual syndrome. Fertil Steril , 62 (2), 313‐
Delara, M., Ghofranipour, F., Azadfallah, P., Tavafian, S. S., Kazemnejad, A., & Montazeri, A. (2012).
Health related quality of life among adolescents with premenstrual disorders: a cross sectional study. Health and Quality of Life Outcomes , 10 (1), 1.
Dennerstein, L., Lehert, P., Bäckström, T., & Heinemann, K. (2010). The effect of premenstrual symptoms
on activities of daily life. Fertil Steril. , 94 (3), 1059‐ 1064.
Dennerstein, L., Lehert, P., Keung, L., Pal, S., & Choi, D. (2010). Asian study of effects of
premenstrual symptoms on activities of daily life. Menopause Int , 16 (4), 146‐ 151.
Freeman, E., Rickels, K., & Yonkers, K. (2001). Venlafaxine in the treatment of premenstrual dysphoric
disorder. Obstet Gynecol , 98, 737‐ 744.
Hallman, J., & Georgiev, N. (1987). The premenstrual syndrome and absence from work due to illness.
Journal of Psychosomatic Obstetrics & Gynecology , 6 (2), 111‐ 119.
Harnett‐ Sheehan, K., & Sheehan, D. (2008). Assessing treatment effects in clinical trials with the Discan
metric of the Sheehan disability Scale. International Clinical Psychopharmacology , 23(2), 70‐ 83.
Hoyer, J., Burmann, I., Kieseler, M.‐ L., Vollrath, F., Hellrung, L., Arelin, K., et al. (2013). Menstrual Cycle
Phase Modulates Emotional Conflict Processing in Women with and without Premenstrual Syndrome (PMS) ‐ A Pilot Study. PLoS ONE , 8 (4).
Kaleli, S. (2001). Symptomatic treatment of premenstrual mastalgia in premenopausal women with lisuride
maleate: A double‐ blind placebo‐ controlled randomized study. Fertil Steril , 75, 718.
Namavar Jahromi, B., Pakmehr, S., & Hagh‐ Shenas, H. (2011). Work Stress, Premenstrual Syndrome and
Dysphoric Disorder: Are There Any Associations? Iranian Red Crescent Medical Journal , 13 (3), 199‐ 202.
International Journal of Innovative Knowledge Concepts, 2(1) January, 2016
Premenstrual Symptoms and Social Disability.
O'Brien. (1987). PMS. Premenstrual syndrome. London: Blackwell Science.
Pearlstein, T., & Steiner, M. (2008). Premenstrual dysphoric disorder: burden of illness and treatment
update. Journal of Psychiatry & Neuroscience?: JPN , 33 (4), 291‐ 301.
Pinar, G., Colak, M., & Oksuz, E. (2011). Premenstrual Syndrome in Turkish college students and its effects on
life quality. Sexual & Reproductive Healthcare , 2 (1), 21‐ 28.
Robinson, R. L., & Swindle, R. W. (2000). Premenstrual Symptom Severity: Impact on Social Functioning
and Treatment‐ Seeking Behaviors. Journal of Women's Health & Gender‐ Based Medicine , 9 (7), 757‐ 768.
Roca, C., Schmidt, P., & Rubinow, D. (1999). A follow‐ up study of premenstrual syndrome. The Journal
of clinical psychiatry , 60 (11), 763‐ 766.
Rubinow, D. R., & Schmidt, P. J. (2006). Gonadal steroid regulation of mood: the lessons of premenstrual
syndrome. Frontiers in neuroendocrinology , 27 (2), 210‐ 216.
Steiner, M., Romano, S., & Babcock, S. (2001). The efficacy of fluoxetine in improving physical symptoms
associated with premenstrual dysphoric disorder. Br J Obstet Gynaecol , 108, 462‐ 468.
Wyatt, K., Paul, D., Peter, J., & P M Shaughn, O. (1999). Efficacy of vitamin B‐ 6 in the treatment of
premenstrual syndrome: systematic review. BMJ , 318, 1375‐ 1381.
Yang, M., Wallenstein, G., Hagan, M., Guo, A., Chang, J., & Kornstein, S. (2008). Burden of premenstrual
dysphoric disorder on health‐ related quality of life. J Womens Health (Larchmt) , 17 (1), 113‐ 121.
Yonkers, K. (2008). Premenstrual syndrome. The Lancet , 371, 1200.
International Journal of Innovative Knowledge Concepts, 2(1) January, 2016
Source: http://www.ijikc.co.in/sites/ijikc/index.php/ijikc/article/view/74/68
JOURNAL OF PLANKTON RESEARCH j VOLUME 32 j NUMBER 10 j PAGES 1405–1411 j 2010 Osmoregulatory and demographicresponses to salinity of the exoticcladoceran Daphnia exilis INGER HEINE-FUSTER 1,2*, CAREN VEGA-RETTER 1,2, PABLO SABAT 2,3 AND RODRIGO RAMOS-JILIBERTO 1,21CENTRO NACIONAL DEL MEDIO AMBIENTE, FUNDACIO´N DE LA UNIVERSIDAD DE CHILE, AV. LARRAI´N 9975, LA REINA, SANTIAGO, CHILE, 2DEPARTAMENTO DE
ORAL APPLIANCES FOR THE TREATMENT OF SNORING AND OBSTRUCTIVE SLEEP APNEA: A REVIEW Oral Appliances for the Treatment of Snoring and ObstructiveSleep Apnea: A ReviewAn American Sleep Disorders Association Review Wolfgang Schmidt-Nowara1, Alan Lowe2, Laurel Wiegand3, Rosalind Cartwright4, Francisco Perez-Guerra5 and Stuart Menn6 1Pulmonary Division, Department of Medicine, University of New Mexico, Albuquerque, NM; 2Department of ClinicalDental Sciences, University of British Columbia, Vancouver, British Columbia, Canada; 3Department of Medicine,Pulmonary/Critical Care Division, Penn State College of Medicine, Hershey, PA; 4Sleep Disorders Service and ResearchCenter, Rush-Presbyterian-St. Luke's Medical Center, Rush University, Chicago, IL; 5Division of Pulmonary Disease, Scottand White Clinic, Temple, TX; and 6Division of Sleep Disorders, Scripps Clinic, La Jolla, CA







