Cpccrn.org

The randomized comparative pediatric critical illness
stress-induced immune suppression (CRISIS) prevention trial
Joseph A. Carcillo, MD; J. Michael Dean, MD; Richard Holubkov, PhD; John Berger, MD; Kathleen L. Meert, MD;K. J. S. Anand, MBBS, DPhil; Jerry Zimmerman, MD, PhD; Christopher J. L. Newth, MB, ChB; Rick Harrison, MD;Jeri Burr, MS, RN-BC; C. C. R. C. Douglas F. Willson, MD; Carol Nicholson, MD
Objectives: Nosocomial infection/sepsis occurs in up to
Measurements and Main Results: There were no differences by
40% of children requiring long-term intensive care. Zinc, se-
assigned treatment in the overall population with respect to time
lenium, glutamine, metoclopramide (a prolactin secretalogue),
until the first episode of nosocomial infection/sepsis (median
and/or whey protein supplementation have been effective in
whey protein 13.2 days vs. zinc, selenium, glutamine, and intra-
reducing infection and sepsis in other populations. We evalu-
venous metoclopramide 12.1 days; p ⴝ .29 by log-rank test) or
ated whether daily nutriceutical supplementation with zinc,
the rate of nosocomial infection/sepsis (4.83/100 days whey pro-
selenium, glutamine, and metoclopramide, compared to whey
tein vs. 4.99/100 days zinc, selenium, glutamine, and intravenous
protein, would reduce the occurrence of nosocomial infection/
metoclopramide; p ⴝ .81). Only 9% of the 293 subjects were
sepsis in this at-risk population.
immunocompromised and there was a reduction in rate of noso-
Design: Randomized, double-blinded, comparative effective-
comial infection/sepsis with zinc, selenium, glutamine, and intra-
ness trial.
venous metoclopramide in this immunocompromised group (6.09/
Setting: Eight pediatric intensive care units in the NICHD Col-
100 days whey protein vs. 1.57/100 days zinc, selenium,
laborative Pediatric Critical Care Research Network.
glutamine, and intravenous metoclopramide; p ⴝ .011).
Patients: Two hundred ninety-three long-term intensive care pa-
Conclusion: Compared with whey protein supplementation,
tients (age 1–17 yrs) expected to require >72 hrs of invasive care.
zinc, selenium, glutamine, and intravenous metoclopramide con-
Interventions: Patients were stratified according to immuno-
ferred no advantage in the immune-competent population. Further
compromised status and center and then were randomly assigned
evaluation of zinc, selenium, glutamine, and intravenous meto-
to receive daily enteral zinc, selenium, glutamine, and intravenous
clopramide supplementation is warranted in the immunocompro-
metoclopramide (n ⴝ 149), or daily enteral whey protein (n ⴝ
mised long-term pediatric intensive care unit patient. (Pediatr Crit
144) and intravenous saline for up to 28 days of intensive care
Care Med 2012; 13:000 – 000)
unit stay. The primary end point was time to development of
KEY WORDS: glutamine; nosocomial infection; prolactin; sele-
nosocomial sepsis/infection. The analysis was intention to treat.
nium; sepsis; whey protein; zinc
Centers for Disease Control
care. Critical illness stress induces lym-
tional supplementation is needed in this
and Prevention recommen-
phopenia and lymphocyte dysfunction as-
population at risk for stress-induced lym-
dations and bundled inter-
sociated with hypoprolactinemia (1) and
phocyte dysfunction and nosocomial in-
ventions for preventing catheter-associ-
also deficiencies in zinc and selenium (2,
ated bloodstream infection, ventilator-
3) and amino acids (4, 5). Because lym-
Metoclopramide, a prolactin secreta-
associated pneumonia, and urinary
phocyte integrity is important for the im-
logue, administered at the dosage com-
catheter-associated infections, nosoco-
mune response to fight infection, stan-
monly used for gastrointestinal prokinesis
mial infection/sepsis remains a signifi-
dard nutritional practice in critically ill
maintains prolactin levels in the high-
cant cause of morbidity in critically ill
children includes zinc, selenium, and
normal range in children. In mechanicallyventilated adults, metoclopramide delayedtime to onset of nosocomial pneumoniaby 50% but had no effect on the rate of
From the Children's Hospital of Pittsburgh of UPMC
of Health and Human Services (DHHS; U10HD050096,
(JAC), Pittsburgh, PA; University of Utah (JMD, RH, JB);
U10HD049981, U10HD500009, U10HD049945,
nosocomial pneumonia or mortality (6).
Children's National Medical Center (JB); Children's
U10HD049983, U10HD050012, and U01HD049934).
In malnourished children, zinc supple-
Hospital of Michigan (KLM); Arkansas Children's Hos-
Members of the Data Safety Monitoring Board
mentation reduced morbidity and mor-
pital (KJSA); Seattle Children's Hospital (JZ); Children's
include Jeffrey R. Fineman, MD, Jeffrey Blumer, PhD,
tality with severe pneumonia (7, 8) or
Hospital Los Angeles (CJLN); University of California at
MD, Thomas P. Green, MD, and David Glidden, PhD.
Los Angeles (RH), Los Angeles, CA; University of Vir-
For information regarding this article, E-mail:
diarrhea (9 –11) and reduced infectious
ginia Children's Hospital (CDFW); and National Institute
disease mortality in small-for-gestation-
of Child Health and Human Development (CN).
Copyright 2011 by the Society of Critical Care
al-age infants (12). Selenium supplemen-
Supported, in part, by the following cooperative
Medicine and the World Federation of Pediatric Inten-
tation (13) or glutamine-enriched enteral
agreements from the Eunice Kennedy Shriver National
sive and Critical Care Societies
nutrition (14) also reduced the risk of
Institute of Child Health and Human Development
(NICHD), National Institutes of Health (NIH), Department
nosocomial sepsis in preterm neonates.
Pediatr Crit Care Med 2012 Vol. 13, No. 4

Enteral glutamine safely maintains T 1
lymphocyte function for bacterial killing(15, 16).
Essential amino acids are also impor-
tant to overall immune function and lym-phocyte function in particular (5). Wheyprotein provides all the essential aminoacids needed to maintain immune func-tion in immune cells. Experimental ani-mal studies show that whey protein sup-plementation facilitates maturation ofthe immune system and is protectiveagainst rotavirus (17–21). Randomizedhuman clinical studies of whey proteinhave demonstrated improved lymphocytefunction and reduction in coinfection inhuman immunodeficiency virus-infectedchildren, reduction in infection in se-verely burned children, and improved im-munologic response to immunization inthe elderly (22–26).
The Eunice Kennedy Shriver National
Institute of Child Health and Human De-velopment Collaborative Pediatric Criti-cal Care Research Network investigatorshypothesized that critical illness stress-induced immune suppression-relatednosocomial infection/sepsis would be
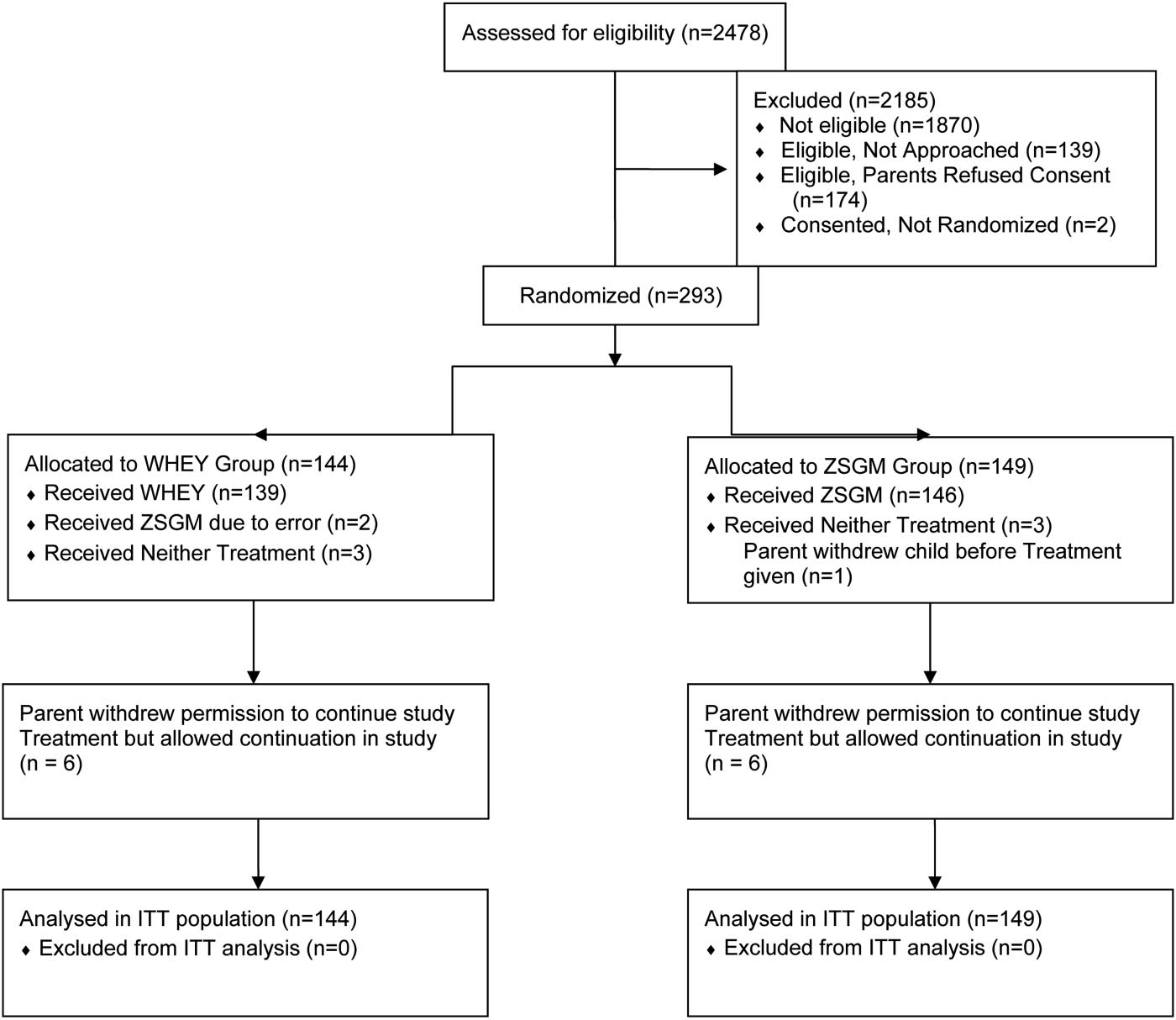
Figure 1. Screening, enrollment, randomization, and study completion.
more effectively prevented by prophylac-tic supplementation of "standard" nutri-
tor (J.M.D.) acted as the sponsor. The study was
Safety Monitoring Board before authorizing
tional practice with added zinc, selenium,
registered with ClinicalTrials.gov (number
enrollment of infants younger than 1 yr. After
glutamine, and metoclopramide, (ZSGM)
the first interim analysis, the Data Safety Mon-
than by prophylactic supplementation
Patients were eligible for enrollment if
itoring Board deferred this authorization until
with added amino acid (whey protein).
they: were older than 1 yr and younger than 18
a second interim analysis could be reviewed.
The Collaborative Pediatric Critical Care
yrs of age; were within the first 48 hrs of PICU
At the time of the second review, the trial was
Research Network designed a random-
admission; had an endotracheal tube, central
terminated for futility. Therefore, no infants
ized, double-blinded, comparative effec-
venous catheter (new or old, tunneled or not
younger than 1 yr were enrolled in the trial.
tiveness trial with the primary hypothesis
tunneled), or urinary catheter; were antici-
The study commenced in April 2007 and ter-
that daily ZSGM would prolong the time
pated to have an indwelling arterial or venous
minated in November 2009.
to development of nosocomial infection/
catheter for blood sampling during the first 3
After informed consent was obtained from
sepsis compared to daily whey protein. In
days of study enrollment; and were anticipated
parents, subjects were randomized by tele-
this article we report the results of the
to have venous access and an enteral feeding
phone according to an a priori design using
critical illness stress-induced immune
tube for the administration of study drugs.
randomized blocks of variable length, strati-
suppression prevention trial.
Patients were excluded from enrollment if
fied according to center and immunocompro-
they: had a known allergy to metoclopramide;
mised status. Immunocompromised status
MATERIALS AND METHODS
were expected to have planned removal of en-
was defined by the known presence of acquired
dotracheal tube, central venous, and urinary
immune deficiency syndrome, cancer, trans-
This randomized, double-blinded, compara-
catheters within 72 hrs after study enroll-
plantation, primary immune deficiency, or
tive study was performed on two parallel groups
ment; had suspected intestinal obstruction;
chronic immune suppressant therapy. Chil-
of children at eight pediatric intensive care units
had intestinal surgery or bowel disruption;
dren were randomized in a 1:1 ratio into the
(PICUs) in the Collaborative Pediatric Critical
had other contraindications to the enteral ad-
two arms of the trial in these stratified groups.
Care Research Network. The Institutional Re-
ministration of drugs or nutrients; received
All patients, medical and nursing staffs, clini-
view Boards of all Collaborative Pediatric Critical
chronic metoclopramide therapy before en-
cal site monitors, and most DCC staff re-
Care Research Network centers approved the
rollment; had a known allergy to whey (cow's
mained blinded throughout the study period.
protocol and informed consent documents. Pa-
milk) or soy-based products; had been dis-
The DCC biostatistician (R.H.) prepared Data
rental permission was provided for each subject.
charged from the PICU in the previous 28
Safety Monitoring Board reports and reviewed
An independent Data Safety Monitoring Board
days; had been previously enrolled in this
results in the two arms but remained blinded
was appointed by the NICHD, and two interim
study; or had a positive pregnancy test. Pa-
to actual group assignment throughout the
safety and efficacy analyses were planned. The
tients were also excluded if their parents indi-
study period. Central and clinical site research
study was performed under an Investigational
cated a lack of commitment to aggressive in-
pharmacists and the pharmacy site monitor
New Drug application from the Food and Drug
tensive care therapies.
were unblinded throughout the study.
Administration (investigational new drug
The Food and Drug Administration re-
Subjects were randomized to receive en-
74,500), for which the DCC Principal Investiga-
quired an interim analysis review by the Data
teral whey protein powder and intravenous
Pediatr Crit Care Med 2012 Vol. 13, No. 4

Table 1. Epidemiologic and clinical characteristics at admission
diatric Critical Care Research Network inves-tigators adjudicated the presence or absence of
Zinc, Selenium, Glutamine,
a nosocomial clinical sepsis or infection event
and Metoclopramide Group
for every subject. Each case was reviewed in-
Group (N ⫽ 144)
dependently by two investigators and pre-sented in detail so that consensus for all out-
Age (yrs), median (range)
comes was attained. All participants in this
Pediatric logistic organ dysfunction, median (range)
adjudication process were blinded to treat-
Pediatric risk of mortality, median (range)
ment arm through the study period.
Organ failure index, median (range)
Secondary outcome variables of this study
Immunocompromised (%)
included the rate of nosocomial infection/sepsis
Postoperative pediatric intensive care unit
per 100 PICU days, number of antibiotic-free
Primary diagnosis (%)
days, incidence of prolonged lymphopenia
(ALC ⱕ1000/mm3 for ⱖ7 days), serum prolac-
tin, zinc, and selenium levels before treatment
and after 7 days of treatment, and the safety
Cardiovascular disease
indicator 28-day mortality and adverse events.
Serum zinc and selenium levels were classified
as deficient if they were below the pediatric
reference ranges of the core laboratory. Zinc
deficiency was defined as a level ⬍0.60 g/mL
Human immunodeficiency virus
in children aged 10 yrs or younger and
g/mL in children aged at least 11 yrs. Sele-
nium deficiency was defined as a level ⬍70
ng/mL in children aged 10 yrs or younger and
⬍95 ng/mL in children aged at least 11 yrs.
Chronic diagnoses (%)
Prolactin deficiency was defined as a level of
Malnutrition (reported as primary or secondary
⬍3 ng/mL across all ages. Glutamine levels
Infection status at entry (%)
were not measured because they are not con-
Existing infection
sidered indicative of total body reserves.
The sample size was calculated to provide
No infection or sepsis
90% power to detect an inverse hazard rate of
Existing lymphopenia (ALC ⱕ1000/mm3)
Baseline core laboratory data (%)
1.5 using a two-sided nonparametric test (log-
rank test) with type I error (␣) of 0.05. This
Prolactin deficiency
required accrual of subjects until 263 had nos-
Selenium deficiency
ocomial events; the estimated total samplesize was 600 subjects based on initial eventrate estimates. A log-rank test with a two-sided
saline (whey protein group) or ZSGM (ZSGM
between admission to the PICU and occur-
␣ ⫽ 0.05, stratified by immune-compromised
group). Subjects assigned to the whey protein
rence of nosocomial infection/clinical sepsis in
status, was used to compare the primary end
group received 0.3 g/kg beneprotein each
PICU patients who have endotracheal tubes,
point of freedom from nosocomial infection or
morning and intravenous saline every 12 hrs.
central venous catheters, or urinary catheters.
sepsis (from time of admission to the PICU
Subjects assigned to the ZSGM group received
Nosocomial events were defined as occurring
until up to 5 days after discharge from the
zinc (20 mg), selenium (40 g age 1–3 yrs,
at least 48 hrs after PICU admission during the
PICU) between treatment arms. Outcome
100 g age 3–5 yrs, 200 g age 5–12 yrs, 400
hospital stay until 5 days after discharge from
rates over time are presented using Kaplan-
g adolescent), and glutamine (0.3 g/kg) each
the PICU; for children remaining in the PICU
Meier freedom from event curves. In the sub-
morning, and intravenous metoclopramide
for ⬎28 days after randomization, events were
group of immunocompromised whey protein
(0.2 mg/kg, maximum 10 mg) every 12 hrs. All
counted until day 33. The study protocol re-
patients, median time to nosocomial infec-
study drugs were shipped from a central phar-
quired that patients be randomized within 48
tion/sepsis was derived at the 50.5% event-free
macy (University of Utah) and dispensed by
hrs of PICU admission and that study drug
site research pharmacists. Subjects received
administration begin within 72 hrs of PICU
study drug until discharge from the PICU or
admission. According to Center for Disease
In prespecified analyses complementary to
for 28 days from the time of randomization,
Control and Prevention definitions, clinical
the primary analysis, rates of infection were
whichever occurred earlier. Enteral drugs
sepsis occurs when patients older than 1 yr
analyzed using Poisson regression analyses,
were administered by feeding tube and discon-
have development of fever (ⱖ38°C), hypoten-
which count multiple events for a single sub-
tinued if the feeding tube was removed or if
sion (ⱕ90 mm Hg), or oliguria (ⱕ20 mL/hr)
ject. Additionally, numbers and proportions of
contraindications to enteral feeding developed
and a clinician initiates antibiotic therapy with
antibiotic-free days during the PICU stay were
during the study. Intravenous drugs were dis-
no positive microbiological evidence and no
compared between study arms using the Wil-
continued if the intravenous was removed.
other recognized cause. Nosocomial infection
coxon rank-sum test. Incidence of prolonged
The hypothesis of the critical illness stress-
occurs when microbiologically (culture, anti-
lymphopenia and all-cause mortality and ad-
induced immune suppression Prevention trial
gen, polymerase chain reaction, or antibody)
verse events at 28 days after randomization
was that daily prophylaxis with enteral zinc,
proven infection is observed in a patient with
were analyzed using the chi-square test or
selenium, and glutamine, and intravenous
fever, hypothermia, chills, or hypotension.
exact analogues when numbers of events were
metoclopramide would delay the time (hours)
The treatment arm blinded Collaborative Pe-
small. Four ZSGM-assigned subjects (one of
Pediatr Crit Care Med 2012 Vol. 13, No. 4

Figure 2. Top, Freedom from nosocomial sepsis according to assigned treatment for all randomized patients. Numbers above the horizontal time axis
denote number of patients remaining at risk at each time point. p ⫽ .29 for log-rank test comparing curves between study arms, stratified by immune
competent status. Middle, Freedom from nosocomial infection/sepsis according to assigned treatment for patients immunocompromised at study entry.
Numbers above the horizontal time axis denote number of patients remaining at risk at each time point. p ⫽ .24 for log-rank test comparing curves between
study arms. Lower, Freedom from nosocomial infection/sepsis according to assigned treatment for patients who were immune-competent at study entry.
Numbers above the horizontal time axis denote number of patients remaining at risk at each time point. p ⫽ .16 for log-rank test comparing curves between
study arms.
whom received no study treatment) had un-
ment, randomization, and study comple-
Treatment with ZSGM did not delay
known 28-day survival status.
tion results.
the time until nosocomial infection/
Five factors (immunocompromised status,
Table 1 shows the epidemiologic and
sepsis compared to treatment with whey
postoperative status, gender, race/ethnicity,
clinical characteristics of the study pop-
protein (median time, whey protein 13.2
and center) were prespecified for subgroup
ulation at the time of enrollment in both
days vs. ZSGM 12.1 days; log-rank p ⫽
analysis, and the Data Safety Monitoring
treatment arms. The median age of chil-
.29; Fig. 2 top). The median PICU stay
Board subsequently added another factor (in-
dren was 7 yrs and ⬍10% were immuno-
was 10 days. Of subjects at risk for an
fection or sepsis at study entry). The inten-
compromised on entry. Baseline charac-
event, approximately 50% in each treat-
tion-to-treat approach was used for all study
teristics were equally distributed between
ment arm were event-free at 14 days after
analyses of efficacy. Analysis by treatment re-
the study arms. Among patients assigned
PICU admission. The effect of immuno-
ceived was performed for the safety outcomes
to whey protein, 46.5% received paren-
compromised status on time to nosoco-
of mortality and occurrence of adverse events.
teral nutrition and 89.6% received en-
mial infection/sepsis was not significant
teral nutrition, compared to 43.0% and
(median time in immunocompromised
90.6% of patients assigned to ZSGM. The
patients, whey protein 10 days vs. ZSGM
We enrolled 293 subjects (Fig. 1). En-
proportion of patients who were allowed
32.4 days; median time in immune com-
rollment was terminated for futility after
nothing by mouth during one or more
petent patients, whey protein 13.2 days
the second interim analysis indicated that
PICU study days was 55% in the whey
vs. ZSGM 11.8 days; p ⫽ .12) for interac-
the conditional power to determine a
protein arm and 53% in the ZSGM arm,
tion between treatment group and immu-
beneficial effect by ZSGM, compared to
with the average proportion of PICU
nocompromised status in the time-to-
the whey protein therapy, was ⬍10%.
study days being allowed nothing by
event analysis (Fig. 2 middle, bottom).
Figure 1 shows the screening, enroll-
mouth at 14% and 13%, respectively.
Other subgroup factors examined were
Pediatr Crit Care Med 2012 Vol. 13, No. 4

Figure 2. Continued.
Pediatr Crit Care Med 2012 Vol. 13, No. 4

Table 2. Rates of nosocomial infection/sepsis, days of invasive lines, urinary catheterization, and
lenium (40% vs. 38%), glutamine (8% vs.
mechanical ventilation by treatment group
7%) primarily as part of routine TPN, andmetoclopramide (3% vs. 5%) for facilita-
Zinc, Selenium, Glutamine,
tion of nasoduodenal tube placement or
and Metoclopramide
gastroesophageal reflux, respectively.
Group (N ⫽ 144)
Group (N ⫽ 149)
Seven-day levels of all three measures
Total events (infection or sepsis)
were significantly higher in ZSGM pa-
Total pediatric intensive care unit days
tients than whey protein patients, and
Total study daysa
change from baseline was also higher
Mean events/patient/100 study days
(p ⬍ .001 for all six comparisons). At 7
95% confidence interval
days, zinc deficiency was present in 19 of
Therapeutic risk factorsDays in pediatric intensive care unit
83 (23%) ZSGM subjects vs. 36 of 80
(45%) whey protein subjects, selenium
Ventilator days (mean/median)
deficiency in 10 of 84 (12%) ZSGM sub-
Central venous catheter days (mean/median)
jects vs. 23 of 80 (29%) whey protein
Endotracheal tube days (mean/median)
subjects, and prolactin deficiency in 3 of
Urinary catheter days (mean/median)
Total ventilator days
84 (4%) ZSGM subjects vs. 14 of 81 (17%)
Total respiratory infections
whey protein subjects. Controlling for
Mean respiratory infections/patient
presence of baseline deficiencies, ZSGM
Per 100 ventilator days (95% confidence interval)
subjects with 7-day measures showed sig-
Total urinary catheter days
Total urinary tract infections
nificantly lower 7-day deficiency rates
Mean urinary tract infections/patient
compared to whey protein subjects for
Per 100 urinary catheter days (95%
zinc (p ⫽ .001 by Cochran-Mantel-
confidence interval)
Haenszel test), selenium (p ⫽ .009), and
Total central venous catheter days
prolactin (p ⫽ .014).
Total bacteremia infections
Mean bacteremia infections/patient
Overall 28-day mortality was 8.1%
Per 100 central venous catheter days (95%
among the 284 children who received
confidence interval)
whey protein or ZSGM and had known28-day status. There was no significant
aStudy days indicates days in pediatric intensive care unit plus additional days after pediatric
difference in 28-day mortality by treat-
intensive care unit discharge that patient was followed-up for events (5 days unless patient was
ment received between whey protein and
discharged from hospital earlier).
ZSGM (8/139 [5.8%] vs. 15/145 [10.3%];p ⫽ .16). Among the 287 children receiv-
not significantly associated with the pri-
treatment arms (Table 2). Distribution of
ing treatment, there were 2624 adverse
mary end point.
events, sites of infection, and infecting
events, including 113 serious adverse
There was no difference in the rate of
organisms were also generally similar be-
events with no significant differences by
nosocomial infection or clinical sepsis
tween the treatment groups (Table 3).
treatment received for whey protein and
per 100 PICU days between the ZSGM and
In the immunocompromised popula-
ZSGM. Among 139 subjects receiving
whey protein groups (Table 2; p ⫽ .81).
tion, the rate of nosocomial infection/
only whey protein treatment, adverse
Examining study days in the PICU, me-
sepsis was reduced in the ZSGM group
events were reported in 126 (90.6%) and
dian number of antibiotic-free days (2 vs.
compared with the whey protein group
serious adverse events were reported in
1; p ⫽ .09) and proportion of days (17%
(unadjusted p ⫽ .006 for interaction be-
37 (26.6%), whereas among 148 subjects
vs. 10%; p ⫽ .19) did not differ between
tween treatment group and immunocom-
receiving ZSGM regimen adverse events
subjects assigned to whey protein vs.
promised status; Table 4). The causes for
were reported in 135 (91.2%) and serious
ZSGM. There was no significant differ-
immune compromise in whey protein
adverse events were reported in 39
ence in the incidence of prolonged lym-
compared to the ZSGM groups were bone
(26.4%). There were also no differences
phopenia (ALC ⱕ1000/mm3 for ⱖ7 days)
marrow transplant two vs. three, other
in specific adverse events, including diar-
between subjects assigned to whey pro-
organ transplant five vs. one, cancer one
rhea (whey protein 12.2% vs. ZSGM
tein (12/144 [8.3%] vs. ZSGM 5/149
vs. three, human immunodeficiency virus
12.2%), dysrhythmias (arrhythmia, extra-
[3.4%]; p ⫽ .07). In the study population,
zero vs. one, severe neutropenia one vs.
systole, nodal rhythm; whey protein 4.3%
41% receiving whey protein and 42% re-
one, chronic high-dose steroids/immune
vs. ZSGM 4.1%), and abnormal move-
ceiving ZSGM had development of noso-
suppressants one vs. three, congenital
ment (akathisia, choreoathetosis, dyski-
comial infection or sepsis. Approximately
immunodeficiency one vs. one, and ther-
nesia, dystonia; whey protein 2.9% vs.
one-third of patients had development of
apeutic hypothermia zero vs. one.
nosocomial infection and one-fifth had
Among subjects with available base-
development of sepsis. Days of invasive
line values, zinc deficiency was present at
lines, urinary catheterization, and me-
baseline in 235 of 280 (84%), selenium
chanical ventilation and rates of site-
deficiency in 156 of 278 (56%), and pro-
Similar to previous literature, we ob-
specific infections based on denominators
lactin deficiency in 68 of 284 (24%) (Ta-
served that nosocomial infection/sepsis
of ventilator days, urinary catheter days,
ble 1). Among whey protein and ZSGM
occurred in ⬎40% of long-term PICU pa-
and central venous catheter days were
subjects, standard of care included the
tients, with ⬍50% of these children be-
not significantly different between the
common use of zinc (44% vs. 39%), se-
ing free from nosocomial infection or
Pediatr Crit Care Med 2012 Vol. 13, No. 4

Table 3. Nosocomial infection/sepsis and sites of nosocomial infection by treatment group
needed, perhaps in a specialized PICUnetwork with a larger immunocompro-
Zinc, Selenium, Glutamine,
mised population, or in a PICU network
and Metoclopramide
with a larger number of centers to prop-
Group (N ⫽ 144)
Group (N ⫽ 149)
erly assess the significance of this signal.
Patients with events
With regard to limitations, several
One or more events (%)
study design and performance variables
Nosocomial infection (%)
require the reader's consideration. First,
Nosocomial sepsis (%)
this trial was performed in the "standard
Site of infection
practice" setting. Protein, zinc, and sele-
Lower respiratory
nium are an accepted part of "standard"
Upper respiratory
pediatric enteral and parenteral nutrition
in the intensive care setting (29, 30) and
Skin or soft tissue
no effort was made to control this nutri-
tional practice. The study results cannotbe applied to patients who are without
any nutrition in the PICU. Second, ourtrial compared the effectiveness of two
Total infecting organisms
nutriceutical strategies to one another,
Candida albicans
rather than to placebo. The research
planning committee wanted to follow
previous study designs of glutamine sup-
Candida glabrata
Candida lusitanae
plementation in newborns that used sin-
gle amino acids as "placebos" to address
Gram-negative bacilli
potential criticism that an apparent effect
in a glutamine arm could be an effect of
protein nutrition rather than of glu-
tamine per se. This rationale is problem-
atic because all amino acids have specific
immune cell effects and therefore are not
Gram-positive bacilli
true placebos (5). Whey protein was the
Gram-negative cocci
only Food and Drug Administration-
approved amino acid supplement avail-
Gram-positive cocci
able to us. Because whey protein is mar-
Staphylococcus coagulase negative
keted as immune nutrition, we designed
a comparative effectiveness trial rather
than a true placebo-controlled trial. A
true placebo arm without any zinc, sele-
nium, or protein was considered outside
of human subjects standards. Two ongoingadult trials comparing the use of a dopa-
sepsis at 14 days and median time to
The ZSGM supplement did not prevent
mine-2 antagonist to placebo in mechani-
nosocomial infection or sepsis being just
persistent lymphopenia or nosocomial in-
cal ventilation and zinc, selenium, and glu-
less than 14 days (27). Similar to previous
fection/sepsis compared with essential
tamine supplements to placebo in severe
reports, we also found a high incidence of
amino acid supplementation from whey
sepsis (NCT0013978, NCT00300391) will
critical illness stress-related zinc and se-
protein in the overall study population.
give information on the effect of these
lenium deficiency, as well as prolactin
We stratified the randomization of pa-
supplements in the absence of concomi-
deficiency in 24% and lymphopenia in
tients to nutriceutical treatment arms ac-
tant protein supplementation. Approxi-
nearly 40% of the patients (1, 28). The
cording to immunocompromised status
mately ten patients in each treatment
observation that nearly 95% of subjects
because we thought it was biologically
arm either did not receive the assigned
had deficiencies at enrollment supports
plausible that the T 2 phenotype-domi-
treatment, or they had their treatments
the study design that used the multi-
nant immunocompromised group of pa-
stopped prematurely on parental request.
modal ZSGM supplement strategy and
tients would benefit differentially from
Post hoc analysis excluding these patients
analyzed the effects on both the pre hoc
ZSGM supplementation. In this regard,
did not change the overall findings of the
stratified immune competent and immu-
we did observe a reduction in the noso-
study. Fourth, a low number of antibiot-
nocompromised populations. We ob-
comial infection/sepsis rate with use of
ic-free days in the subjects enrolled in
served more frequent resolution of zinc,
ZSGM in this at-risk population. Because
either arm of this study was discovered.
selenium, and prolactin deficiencies at 7
⬍10% of our general PICU population This calls into question whether high an-
days with ZSGM, but this pharmacoki-
was immunocompromised, the small
tibiotic use diminished any effects of the
netic effect was not matched with the
sample size leads us to view these find-
nutriceuticals. However, post hoc analy-
hypothesized pharmacodynamic effect.
ings rather cautiously. Repeated study is
sis found no association between extent
Pediatr Crit Care Med 2012 Vol. 13, No. 4
Table 4. Rates of nosocomial infection/sepsis per 100 days by treatment group and immunocompro-
immune system during zinc deficiency.
Annu Rev Nutr 2004; 24:277–298
3. Stone CA, Kawai K, Kupka R, et al: Role of
Zinc, Selenium, Glutamine,
selenium in HIV infection. Nutr Rev 2010;
and Metoclopramide
4. Roth E: Immune and cell modulation by
amino acids. Clin Nutr 2007; 26:535–544
5. Li P, Yin YL, Li D, et al: Amino acids and
Total events (infection or sepsis)
immune function. Br J Nutr 2007; 98:
Total pediatric intensive care unit days
6. Yavagal DR, Karnad DR, Oak JL: Metoclopra-
Mean events/patient/100 study days
6.09 (3.33–10.32)
1.57 (0.53–3.73)
mide for preventing pneumonia in critically
(95% confidence interval)
ill patients receiving enteral tube feeding: Arandomized controlled trial. Crit Care Med
Zinc, Selenium, Glutamine,
2000; 28:1408 –1411
and Metoclopramide
7. Brooks WA, Yunus M, Santosham M, et al:
Group (N ⫽ 133)
group (N ⫽ 135)
Zinc for severe pneumonia in very young
children: Double-blind placebo-controlled
Total events (infection or sepsis)
trial. Lancet 2004; 363:1683–1688
Total pediatric intensive care unit days
8. Fischer Walker C, Black RE: Zinc and the
risk for infectious disease. Annu Rev Nutr
Mean events/patient/100 study days
4.72 (3.87–5.69)
5.44 (4.47–6.55)
2004; 24:255–275
(95% confidence interval)
9. Baqui AH, Black RE, El Arifeen S, et al: Zinc
therapy for diarrhoea increased the use oforal rehydration therapy and reduced the useof antibiotics in Bangladeshi children.
of antibiotic use and evidence of treat-
(Data Coordinating Center), Salt Lake
J Health Popul Nutr 2004; 22:440 – 442
ment effect.
City, UT: J. Michael Dean, MD, MBA, Jeri
10. Bhatnagar S, Bahl R, Sharma PK, et al: Zinc
Burr, MS, RN-BC, CCRC, Amy Donald-
with oral rehydration therapy reduces stool
son, MS, Richard Holubkov, PhD, Angie
output and duration of diarrhea in hospital-
Webster, MStat, Stephanie Bisping, RN,
ized children: A randomized controlled trial.
Nosocomial infection and sepsis re-
Teresa Liu, MPH, Brandon Jorgenson,
J Pediatr Gastroenterol Nutr 2004; 38:34 – 40
mains a prevalent public health problem
BS, Rene Enriquez, BS, Jeff Yearley, BS;
11. Raqib R, Roy SK, Rahman MJ, et al: Effect of
in critically ill children with long-term
Children's National Medical Center, WA
zinc supplementation on immune and in-
stay in the PICU. Implementation of Cen-
DC: John Berger, MD, Angela Wratney,
flammatory responses in pediatric patients
ters for Disease Control and Prevention-
MD, Jean Reardon, BSN, RN; Children's
with shigellosis. Am J Clin Nutr 2004; 79:
recommended practices is the first step in
Hospital of Michigan, Detroit, MI: Kath-
prevention. Our study was performed on
leen L. Meert, MD, Sabrina Heidemann,
12. Sazawal S, Black RE, Menon VP, et al: Zinc
the premise that evaluation of the com-
supplementation in infants born small for
MD, Maureen Frey, PhD, RN; Arkansas
parative effectiveness of prophylactic nu-
gestational age reduces mortality: A prospec-
Children's Hospital, Little Rock, AR: KJS
tritional support strategies could inform
tive, randomized, controlled trial. Pediatrics
Anand, MBBS, DPhil, Parthak Prodhan,
further improvement. The novel multi-
2001; 108:1280 –1286
MD, Glenda Hefley, MNSc, RN; Seattle
13. Darlow BA, Austin NC: Selenium supplemen-
modal strategy designed and used to re-
Children's Hospital, Seattle, WA: Jerry
tation to prevent short-term morbidity in
duce critical illness stress-induced zinc,
Zimmerman, MD, PhD, David Jardine,
preterm neonates. Cochrane Database Syst
selenium, glutamine, and prolactin defi-
MD, Ruth Barker, RRT; Children's Hospi-
Rev 2003; 4:CD003312
ciencies was successful in part in revers-
tal Los Angeles, Los Angeles, CA: Chris-
14. van den Berg A, van Elburg RM, Westerbeek
ing these deficiencies. It conferred no ad-
topher J. L. Newth, MB, ChB, J. Francisco
EA, et al: Glutamine-enriched enteral nutri-
vantage in nosocomial infection and
Fajardo, CLS (ASCP), RN, MD; Mattel
tion in very-low-birth-weight infants and ef-
sepsis prevention in immune-competent
Children's Hospital at University of Cali-
fects on feeding tolerance and infectious
children compared to whey-based amino
fornia Los Angeles, Los Angeles, CA: Rick
morbidity: A randomized controlled trial.
acid supplementation. Further study of
Harrison, MD; University of Virginia Chil-
Am J Clin Nutr 2005; 81:1397–1404
the ability of ZSGM supplementation to
15. Boelens PG, Houdijk AP, Fonk JC, et al: Glu-
dren's Hospital, Charlottesville VA: Doug-
prevent nosocomial infection and sepsis
tamine-enriched enteral nutrition increases
las F. Willson, MD; National Institute of
in the immunocompromised PICU popu-
in vitro interferon-gamma production but
Child Health and Human Development,
lation is warranted.
does not influence the in vivo specific anti-
Bethesda, MD: Carol Nicholson, MD,
body response to KLH after severe trauma. A
Tammara Jenkins, MSN RN.
prospective, double blind, randomized clini-
cal study. Clin Nutr 2004; 23:391– 400
16. Yalcin SS, Yurdakok K, Tezcan I, et al. Effect
Members of the Collaborative Pediat-
of glutamine supplementation on diarrhea,
ric Critical Care Research Network par-
1. Felmet KA, Hall MW, Clark RS, et al: Pro-
interleukin-8 and secretory immunoglobulin
ticipating in this study: Children's Hospi-
longed lymphopenia, lymphoid depletion,
A in children with acute diarrhea. J Pediatr
tal of Pittsburgh, Pittsburgh, PA: Joseph
and hypoprolactinemia in children with nos-
Gastroenterol Nutr 2004; 38:494 –501
Carcillo, MD, Michael Bell, MD, Alan
ocomial sepsis and multiple organ failure.
17. Ha E, Zemel MB: Functional properties of
Abraham, BA, Annette Seelhorst, RN,
J Immunol 2005; 174:3765–3772
whey, whey components, and essential
Jennifer Jones RN; University of Utah
2. Fraker PJ, King LE: Reprogramming of the
amino acids: mechanisms underlying health
Pediatr Crit Care Med 2012 Vol. 13, No. 4
benefits for active people (review). J Nutr
effects of dietary whey proteins in mice.
26. Freeman SL, Fisher L, German JB, et al:
Biochem 2003; 14:251–258
J Dairy Res 1995; 62:359 –368
Dairy proteins and the response to pneu-
18. Low PP, Rutherfurd KJ, Gill HS, et al: Effect
22. Micke P, Beeh KM, Buhl R: Effects of long-
movax in senior citizens: A randomized, dou-
of dietary whey protein concentrate on pri-
term supplementation with whey proteins on
ble-blind, placebo-controlled pilot study. Ann
mary and secondary antibody responses in
plasma glutathione levels of HIV-infected pa-
N Y Acad Sci 2010; 1190:97–103
immunized BALB/c mice. Int Immunophar-
tients. Eur J Nutr 2002; 41:12–18
27. Leclerc F, Leteutre S, Duhamel A, et al: Cu-
macol 2003; 3:393– 401
23. Micke P, Beeh KM, Schlaak JF, et al: Oral
mulative influence of organ dysfunctions and
19. Perez-Cano FJ, Marin-Gallen S, Castell M, et
supplementation with whey proteins in-
septic state on mortality of critically ill chil-
al: Supplementing suckling rats with whey
creases plasma glutathione levels of HIV-
dren. Am J Resp Crit Care Med 2005; 171:
protein concentrate modulates the immune
infected patients. Eur J Clin Invest 2001;
response and ameliorates rat rotavirus-
28. Skelton JA, Havens PL, Werlin JL: Nutrient
induced diarrhea. J Nutr 2008; 138:
24. Moreno YF, Sgarbieri VC, da Silva MN, et al:
deficiencies in tube fed children. Clin Pediatr
Features of whey protein concentrate supple-
2006; 45:37– 41
20. Perez-Cano FJ, Marin-Gallen S, Castell M, et
mentation in children with rapidly progressive
29. Jeejeebhoy K: Zinc essential trace element
al: Bovine whey protein concentrate supple-
HIV infection. J Trop Pediatr 2006; 52:34 –38
for parenteral nutrition. Gastroenterology
mentation modulates maturation of immune
25. Alexander JW, MacMillan BG, Stinnett JD, et
2009; 137(5 Suppl):S7–S12
system in suckling rats. Br J Nutr 2007;
al: Beneficial effects of aggressive protein
30. Shenkin A: Selenium in intravenous nutri-
98(Suppl 1):S80 –S84
feeding in severely burned children. Ann
tion. Gastroenterology 2009; 137(Suppl 5):
21. Wong CW, Watson DL: Immunomodulatory
Surg 1980; 192:505–517
Pediatr Crit Care Med 2012 Vol. 13, No. 4
Source: http://www.cpccrn.org/documents/PediatrCritCare2012Carcillo.pdf
Caregiver Lifeline Program Resources for Transplant Families This document is a good starting point for identifying potential transplant-related resources for patients, their caregivers and families. We've included a variety of information about transplant, transplant fundraising resources, grant assistance providers, travel assistance, prescription coverage, and living donor support.
Volume 2, Number 1, June 2009 ISSN 1995-6681 Pages 1 -6 Jordan Journal of Earth and Environmental Sciences Diurnal and Seasonal Variation of Air Pollution at Al-Hashimeya Sana'a Abed El-Raoof Odat * Department of Earth Science and Environment, Faculty of Natural Resources and Environment,Hashemite University, Jordan Abstract







