Harmony.cl
Lasers Med SciDOI 10.1007/s10103-008-0545-3
Results of fractional ablative facial skin resurfacingwith the erbium:yttrium-aluminium-garnet laser 1 weekand 2 months after one single treatment in 30 patients
Mario A. Trelles & Serge Mordon & Mariano Velez &Fernando Urdiales & Jean Luc Levy
Received: 13 December 2007 / Accepted: 17 January 2008
# Springer-Verlag London Limited 2008
Abstract The erbium:yttrium-aluminium-garnet (Er:YAG)
were no side effects except for in one phototype IV patient,
laser has recently been used in the fractional resurfacing of
who had hyperpigmentation. Histology 2 months after the
photo-aged skin. Our study evaluated the results after one
single treatment demonstrated younger morphology of both
single session of
fractional resurfacing with Er:YAG.
the epidermis and dermis, with improvement of the pre-
Thirty women participated in the study, with an average age
treatment typical elastotic appearance. At the parameters
of 46 years, skin types from II to IV, and wrinkle grades I to
used in our study, only one treatment session of Er:YAG
III. The 2,940 nm Er:YAG system used (Pixel, Alma Laser,
laser could achieve effective skin rejuvenation, with effects
Israel) had variable pulse durations (1 ms to 2 ms) and
recognized in both the dermis and, more importantly, the
energy densities (800 mJ/cm2 to 1,400 mJ/cm2) which,
epidermis. This regimen offers an interesting alternative
together with the number of passes (four to eight), were
to the conventional approach of multi-session fractional
selected as a function of wrinkle severity. All patients
received only one treatment. Postoperative side effects wereevaluated. The number of wrinkles was documented with
Keywords Laser surgery . Fractional resurfacing .
clinical photography and was scored. Histological assess-
Er:YAG laser . Skin . Histology
ment was carried out on two patients before and 2 monthsafter treatment. All patients completed the study. Of thepatients, 93% reported good or very good improvement of
the degree of their wrinkles, with a satisfaction index of83%. Pain was not a problem during treatment, and there
Laser ablative resurfacing remains the "gold standard" forrejuvenating severely photo-damaged facial skin, but it isassociated with long-term sequelae-related patient down-time. Recently, fractional resurfacing has been introduced
M. A. Trelles
: M. VelezInstituto Medico Vilafortuny, Fundacion Antoni de Gimbernat,
in the armamentarium of the dermatologist's equipment.
Fractional resurfacing employs a unique mechanism ofaction that repairs a fraction of skin at a time. The laser is
S. Mordon (
*)
used to resurface the epidermis and, at the same time, to
INSERM U703, IFR 114, Pavillon Vancostenobel,Lille University Hospital, CH&U,
heat the dermis to promote safely the formation of new
59037 Lille, France
collagen. The untreated healthy skin remains intact and
actually aids the repair process, promoting rapid healingwith only a day or two of downtime. Various modalities of
F. UrdialesInstituto Médico Miramar,
"fractional" resurfacing have been offered as alternatives to
laser ablative resurfacing, designed to decrease the photo-thermal side effects while still achieving good results, with
faster healing of the skin and significant reductions in
Centre Laser Dermatologique,Marseille, France
Irrespective of the laser wavelength used in the fractional
with moderate elastosis (visible translucent yellow papules
system, the primary target is both the epidermis and the
under direct lighting) and some dyschromia. Type III
dermis, with the aim of creating small zones of "micro-
wrinkles were defined as a large number of fine-to-
damage" separated by zones of unirradiated tissue that
moderately deep wrinkles at rest, and very deep wrinkles
assist with the rapid healing process. The aim of the
with motion in association with severe elastosis and
fractional approach is to obtain the best possible results
thickened yellow multipapular skin under direct lighting,
with the least possible damage, and the degree of thermal
coarse on palpation and with a significant number of
damage delivered to the target skin depends on the dosage,
dyschromic lesions.
the pulse width of the beam, and the number of passes over
Exclusion criteria for treatment included pregnancy,
the same target area. A fractional system based on the
nursing, inflammatory skin diseases, open wounds, active
erbium:yttrium-aluminium-garnet (Er:YAG) laser has recently
herpes simplex, facial congenital/acquired naevi, and
become commercially available. When the Er:YAG laser is
refusal to give signed informed consent.
used for resurfacing in the fractional mode, recovery time is
Treatment details were explained to each patient, and all
considerably shortened and traditional post-resurfacing se-
signed a form of informed consent for surgery and the use
quelae are absent. Consequently, this allows patients a rapid
of clinical photography. The study was approved by the
return to their social or work environments. Debate continues
Antoni de Gimbernat Foundation Ethics Committee.
on the use of multiple treatment sessions or one single
The laser used was the Pixel Er:YAG system (Harmony
treatment session. From our study we present the results
platform, Alma Laser, Israel) equipped with a beam splitter
obtained from 30 patients and the associated symptoms
to divide the 2,940 nm beam into several sets of microbeams.
observed after a single session of fractional resurfacing by
The window of the laser handpiece was 11 mm×11 mm,
multi-pass Er:YAG laser.
supporting 49 microbeams. The system has three pro-grammes for treatment pulse width: short (1 ms pulse width),medium (1.5 ms) and long (2 ms).
Materials and methods
The energy programme for fractional resurfacing with
this fractional Er:YAG laser is based on a variable pulse
Patients and treatment
width at a fixed output power. Depending on selection ofthe short, medium or long pulse setting, the radiant
Thirty women participated in the study, with ages ranging
exposures over the entire 11 mm×11 mm treatment area
from 25 years to 52 years (mean age 46 years). Three
are 800 mJ/cm2, 1,000 mJ/cm2 and 1,400 mJ/cm2,
patients underwent full face resurfacing, eight, periocular
respectively. The manufacturer's recommendation is that
and 19, upper lip. Four patients were skin phototype II; 18,
treatment can be given without the use of anaesthesia for all
type III and eight, type IV. Fifteen patients presented with
programmes, but, in clinical practice, repeated passes with
degree III wrinkles, 11 degree II, and four degree I
the system with small inter-shot intervals over the same
(Table Tables and show the wrinkle grade broken
area inevitably leads to heat accumulation, especially when
down by the area to be treated and the fractional ablative
the long pulse option (1,400 mJ/cm2) is chosen, and, as a
resurfacing pulse programme chosen.
consequence, some degree of pain will be experienced,
For inclusion in the study, patients were limited to those
directly correlated with the number of laser passes. In our
with wrinkles between degrees I and III, based on the
study, application of the long pulse setting for type III wrinkles
Glogau scale. Type I wrinkles were defined as fine, seen
was preceded by the administration of local anaesthesia (4%
with motion in association with mild elastosis, fine textural
lidocaine in suspension, Laboratorios Profarplan, Barcelona,
changes and a subtle accent of skin lines. Type II wrinkles
Spain) applied topically 2 h prior to surgery. The excess
were defined as a moderate number of fine wrinkles at rest,
anaesthetic was removed and the skin surface cleaned. The
plus moderate-to-deep wrinkles with motion in association
Table 2 Patients broken down by area treated and wrinkle grade. The
Table 1 Patients (total = 30) broken down by age group, skin
upper lip accounted for the largest number of patients with grade III
phototype and wrinkle grade (Glogau scale). Grade III wrinkles were
wrinkles in 50% of all patients
treated with the long pulse programme and grade II and grade Iwrinkles were treated with the medium and short pulse programmes,
25-32 years 33-34 years 45-52 years II III IV I
Table 3 Results correlated with wrinkle site and grade and pulse
patients were advised to begin their normal regimen of skin
programme as evaluated by patients at the 2-month assessment point
care and creams following the spontaneous detachment of
the scab. Advice was also given regarding the avoidance ofsolar exposure, and the use of a UVA/B sun block with a
solar protection factor 60 (SPF 60) was recommended.
Two patients from each of the three pulse width groups, as
a trial population cross-section, volunteered to have 0.5 mm
punch biopsies taken from the treatment area before and
2 months after treatment. Clinical photography ensured that
the same biopsy point was not used more than once.
Patients were asked to record information regarding
procedure-related pain and other postoperative side effects
such as erythema and hyperpigmentation. Patients were
instructed on how to score procedure-related pain using an
+++ Very much less, ++ much less, + somewhat less, ± little or no
11-point visual analogue scale (VAS), where 10 was unbear-
improvement, − worse
able pain and zero was no pain, and the results were graded asfollows: extremely painful (10–9 on the VAS, +++); very
laser was fired eight times, maintaining the head over the same
painful (7–8, ++); bearable pain (6–4, +); little pain (1–3, ±);
area but turning it slightly around its perpendicular axis each
and no pain (0, −) Answers were tabulated. At the 7-day and
time. Consequently, this technique corresponded to eight
2-month points the patients subjectively assessed erythema
passes. Once the laser had been fired eight times, the
and hyperpigmentation (severe, +++; bad, ++; noticeable, +;
handpiece was moved to another treatment area. In patients
mild, ±; and none, −); changes in their lines and wrinkles (very
with types I or II wrinkles, where lighter fractional resurfacing
much less, +++; much less, ++; somewhat less, +; little or no
was required, no anaesthesia was used and the programme
change, ±; and worse, −); and the overall treatment efficacy
was set to the short pulse mode (800 mJ/cm2) with four
based on the result as a whole (excellent, +++; good, ++;
passes, or medium pulse mode (1,000 mJ/cm2) with six
fair, +; little or no change, ±; and worse, −). The patients'
passes, respectively (Table ) depending on the severity
satisfaction at the 2-month assessment, based on the improve-
of the wrinkles. All patients, regardless of the degree of
ment in lines, wrinkles and general skin condition, was graded
wrinkles, received only one treatment.
as very satisfied (VS); satisfied (S); somewhat satisfied (FS);
Standardized digital photographs (Sony MAVICA
and not satisfied (NS). The values scored for VS and S were
MVC-FD91) were taken of the patients' skin condition
summed and expressed as a percentage to give the patient
before the treatment (baseline assessment) and then 7 days
satisfaction index (SI). The efficacy of Er:YAG fractional
and 2 months after treatment (7-day and 2-month assess-
resurfacing for skin rejuvenation was assessed objectively
ments), maintaining uniformity in the patient's position, the
from the clinical photography at baseline, 7 days, and
lighting and the camera set-up. A separate floppy disk was
2 months after treatment, by two independent expert and
kept for each patient to enable accurate repetition of the
blinded aesthetic dermatologists. Where their assessment
photography and follow-up. The clinical photography
dramatically differed, consensus was reached after discussion.
allowed comparative assessment of the state of lines,
Grading was as follows: excellent improvement, +++ (85–
wrinkles and skin condition over the three assessment
100%); good improvement, ++ (60–84%); fair improve-
points. Following the fractional resurfacing, flupametasone
ment, + (30–59%); little or no improvement, ± (0–29%); and
gentamicin ointment (Flutenal Gentamicina, Lab. Recordati
España, S.L., Madrid, Spain) was gently applied to the
The histological specimens taken at baseline and at the
treated area. No occlusive dressing was used. Patients were
2-month assessment were stained with haematoxylin and
recommended to use the ointment three times a day in small
eosin (H&E), and an independent and blinded pathologist
amounts (as a moisturizer), until spontaneous detachment
was asked to comment on any changes seen in the
of the scab that would form on the treated areas. No oral
epidermal and dermal architecture.
medication was prescribed, but patients were advised totake paracetamol, 500 mg every 4 h, if pain occurred.
All patients completed the trial and participated in the two
Patients were asked to return 24 h after treatment for control,
assessments. During Er:YAG fractional resurfacing, all
and 7 days and 2 months after treatment for evaluation. All
patients treated with the long pulse programme reported
increased discomfort with some pain with the eight laser
2-month assessments with the original wrinkle grade.
passes, despite the application of the topical local anaes-
Increased improvement in all grades was seen at the final
thetic. In particular, pain was experienced from the fifth
assessment point.
pass onwards and when the treatment was for the full face.
Procedure-related pain is described in Table , and the
However, no patient refused to finish the treatment. On the
majority of patients found the procedure somewhat painful
other hand, all patients treated with the short and medium
(20/80), although no patient found the pain unbearable. On
pulse programmes also experienced some discomfort with
the other hand, no patient was totally pain free. Table also
noticeable pain, but again no patient refused to continue
shows the degrees of erythema and hyperpigmentation at
with the treatment.
the 7-day assessment point, which are perhaps difficult for
One day after surgery patients treated with the short and
patients to assess because of inter-individual subjective
medium pulse programmes presented with skin irritation.
variations. Although none found severe erythema,12 of the
Some erythema was present, with slight scabbing that
30 patients felt their erythema was bad at post-treatment
spontaneously detached after approximately 4 or 5 days,
day 7, and the remaining graded it as noticeable to mild. No
sooner than was the case following treatment with the long
patient was erythema free. Some degree of hyperpigmen-
pulse programme. Once the skin was free of the small fine
tation was seen in three patients, with none seen in the
scab in all treatment groups, erythema was more apparent,
remaining 27. Table further shows the evolution of
but the reaction was much less than when compared with
erythema and hyperpigmentation between the two assess-
standard ablative laser resurfacing, according to the opinion
ment points and among skin types, from which it can be
given by the clinical personnel involved in and familiar
seen that erythema had completely evolved by the final
with ablative resurfacing treatments. Patients treated with
assessment in all skin types. In nearly all patients it had, in
the long pulse programme presented with oedema and
fact, evolved by 2 weeks after treatment: camouflage make-
slight exudation the day after resurfacing but reported a
up was recommended in the few cases in which it persisted
mild ache with almost no discomfort. Seven days after Er:
beyond the 2-week mark. Hyperpigmentation spontaneous-
YAG fractional resurfacing, scabbing had almost totally
ly resolved in all skin types by the 2-month assessment,
disappeared in all 30 patients, with detachment of the crust
except for one type IV patient treated with the long pulse
occurring between days 3 and 4 for the short pulse
programme. No other complication, such as scarring,
programme, around day 5 for the medium pulse programme
developed in any of the subjects, but one skin type II
and between days 6 and 7 for the long pulse programme. The
patient, treated on the upper lip, developed herpes simplex
intensity of the erythema was directly correlated with the
seen at the 7-day assessment, which was possibly related to
length of the treatment pulse. The new skin was fine and fresh-
the too-early application of camouflage makeup but which
looking in all cases, and fine lines had disappeared.
had completely resolved by the 2-month assessment. It
Table correlates the subjective assessment of the
should be noted here that prophylactic anti-herpes agents
results achieved at the 2-month assessment point, broken
were not used at all in this study.
down by both treatment programme and treated area. The
The comparison between the patients' and clinicians'
majority of patients were treated on the upper lip (19/30),
assessments of efficacy can be seen in Table , for the 7-
followed by periocular (8/30) and full face resurfacing
day and 2-month assessments. Both clinicians concurred in
(3/30). Best results were for the full face and the upper lip
all assessments. Although the clinicians' assessments
compared with periocular resurfacing, although this might
tended to be more favourable than the subjective patients'
have been a function of patient numbers. Table correlates
scores, they correlated very well. The one patient who rated
the improvement in lines and wrinkles at the 7-day and
herself worse at the 2-month assessment was the long
Table 5 Degree of procedure-related pain, and erythema and
Table 4 Patients' subjective changes in lines and wrinkles at the 7-
pigmentation (7-day assessment)
day and 2-month assessment points, by wrinkle grade
Pain grade: +++, extremely painful (10–9 on the VAS); ++, verypainful (7–8); +, bearable (6–4); ±, little pain (1–3); –, no pain (0)
+++ Very much less, ++ much less, + somewhat less, ± little or no
Erythema and pigmentation: +++, severe; ++, bad: +, noticeable; ±,
improvement, − worse
Table 6 Erythema and hyperpigmentation at the 7-day and 2-month
Table 8 Patient satisfaction grades and numbers at 7 days and 2
assessments, correlated with patients' skin types
months after fractional Er:YAG resurfacing
Assessment points
Number of patients
+++, Severe; ++, bad; +, noticeable; ±, mild; —, none
VS very satisfied; S satisfied; SS fairly satisfied; NS not satisfiedSatisfaction indices for the 7-day and 2- month assessments (SI,calculated by adding the VS and S values expressed as a percentage of
pulse-treated type IV patient in whom hyperpigmentation
the patient population) were 63.3% and 83.3%, respectively.
had persisted. In both the patients' and clinicians' assess-ments, improved scores were apparent at the final assess-
ment compared with the 7-day assessment, which is inagreement with all previous resurfacing and rejuvenation
The aim of our carrying out only one treatment and not
studies having a longer-term follow-up.
various sessions of treatment, as is usually recommended in
Subjective patient satisfaction grades and numbers 7
fractional resurfacing, was to meet patient compliance to
days and 2 months after fractional Er:YAG resurfacing are
the maximum and to achieve the best possible skin
seen in Table . The satisfaction indices (SI, calculated by
improvement, while still respecting safety aspects and
the addition of VS and S values and expressed as a
obtaining rapid tissue recovery. Treatment was not only to
percentage of the patient population) for the 7-day and 2-
improve the appearance of wrinkles, but comprehensively
month assessments were 63.3% and 83.3%, respectively,
to remove other symptoms of photo-aging, meeting all the
once again showing an improved SI for the longer follow-up.
criteria of "skin rejuvenation" as proposed by Bitter [].
Typical histological findings at baseline and at the 2-
To achieve this, our goal was to gain as much of an
month assessment are shown in Fig. , and typical
effect as possible in one treatment but with controlled
examples of clinical photographic evidence before treat-
photothermal reactions, so that patients could rapidly re-
ment and 7 days and 2 months after treatment are
incorporate their daily activities. At the same time, in those
illustrative of the results and progression in time of the
patients presenting with degree III wrinkles, we sought to
various degrees of wrinkles treated in Figs. and The
leave enough thermal damage with one treatment to
patient who contracted herpes simplex is seen in Fig. but
subsequently stimulate the underlying dermis, thereby
the improvement in her wrinkles should also be noted.
triggering collagen formation through the wound healingprocess.
The thermal effects of Er:YAG laser can be substantially
Table 7 Subjective (patient) and combined objective (clinician)
enhanced when treatment is carried out with sub-ablative
efficacy scored at the 7-day and 2-month assessments after single-
energies []. As a result of eight passes, in the case of skin
session fractional Er:YAG resurfacing (by numbers of patients)
presenting with grade III wrinkles in the treatment with the
long pulse programme, heat accumulated in the epidermiswith repeated passes having a small interpulse interval and
reached the underlying dermis in the form of conducted
heat. On the other hand, one or two laser passes withfractional Er:YAG laser resurfacing produced a very mild
epidermal micro-peel, with minimal or no thermal propa-
gation to the dermis. This was the aim in the treatment of
grade I wrinkles with the short pulse programme. When
patients presented with grade II wrinkles, the medium pulse
programme was used. In principle, when fractional resur-
Patient: +++, excellent; ++, good; +, fair; ±, little or no change; −,
facing with Er:YAG laser is carried out with various
worse. Doctors: +++, excellent improvement (85–100%) ; ++, good
combinations of passes, the epidermis can be removed
improvement (60–84%); +, fair improvement (30–59%); ±, little or noimprovement (0–29%); −, worse
precisely and progressively and the skin takes only a few
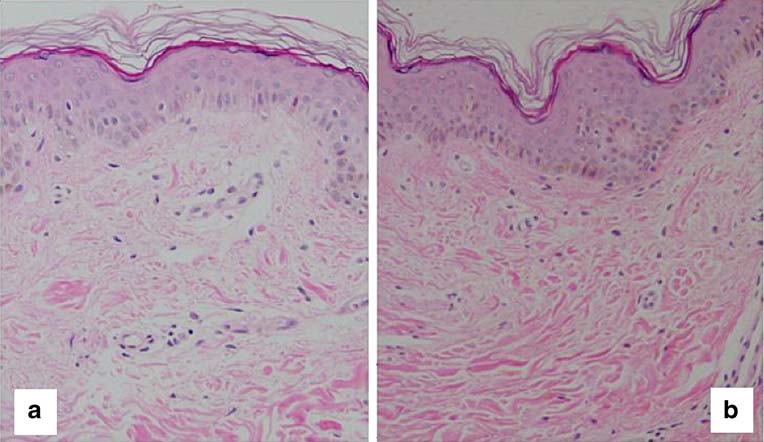

Fig. 1 Skin before (a) and 2 months after (b) a single treatment
skin, with a multicellular wavy epidermis. The dermo-epidermal
(1,400 mJ, eight passes). A Dense keratin on a typical photo-aged
junction is well defined, with fine collagen fibres, well organized
epidermis and dermis. The basal epidermal layer is not well defined,
linearly, in the superficial dermis running parallel and attached to the
and, in the dermis, there is lack of fibre organization and noticeable
basement membrane. In general, the collagen fibres are more compact
interfibrillary spaces typical of the elastosis phenomenon. (b) Two
and with fewer interfibrillary spaces. Both H&E, ×4
months after, the tissue aspect is more in accordance with a younger
days to heal. With only a few laser passes, improvement
wound healing process brought into play by the thermal
occurs in the "dull" appearance of a photo-aged epidermis
damage in the dermis [].
but with little repercussion in the dermis because of the low
To achieve the maximum possible effect with only one
level of conducted heat deposited there. As a result, this
treatment, we chose the long pulse programme in eight
will not have any real effect on wrinkles. On the other hand,
passes to produce better skin results regarding wrinkles.
several Er:YAG passes during fractional resurfacing, with
Multiple passes, with the long pulse programme, in only
the higher energy of the long pulse programme, will peel
one treatment could be thought of as "more aggressive"
the skin more deeply, deposit much more heat into the
than has been previously reported in studies ]. Howev-
dermis to give the required residual thermal damage, and
er, we believe that the treatment as described not only
will thus bring about beneficial morphological changes to
changes the aspect of the epidermis but increases the level
both the epidermis and the superficial dermis due to the
of photothermal dermal irritation via heat propagation to
Fig. 2 Caucasian woman, 50years old, phototype III, (a)before and (b) after full-facefractional resurfacing with Er:YAG laser (1,400 mJ, eightpasses, only one treatment);details of the periocular area areemphasized in order to show theimprovement of wrinkles andskin texture, lightening and re-juvenation of the whole aspectof the skin. c The patient duringtreatment
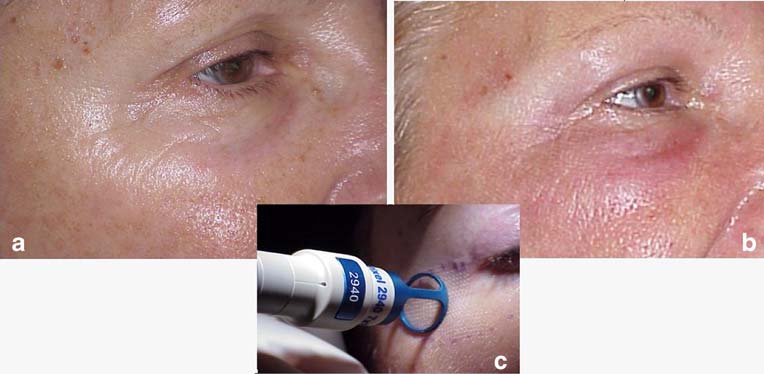

Fig. 3 Caucasian woman, 52years old, skin phototype IV,(a) before and (b) after periocu-lar resurfacing (1,400 mJ, eightpasses, one treatment). Observethe better skin condition andfewer wrinkles at the 2-monthassessment point. c Duringtreatment
affect the dermis. The primary action achieved by the Er:
long pulse is required, with a larger number of passes, so
YAG resurfacing treatment is epidermis renewal, but the
that the resurfaced epidermis has the "younger" appearance
stacking of passes deposits sufficient heat in the dermis to
essential in skin rejuvenation, but it is accompanied by a
stimulate neocollagenesis, which is essential to provide the
significant improvement in the appearance of wrinkles due
result both the clinician and patient require, because the
to good reorganization and tightening of the extracellular
architecture of both the epidermis and the dermis is
matrix. Grade III patients must, therefore, be more prepared
improved. In fact, the external aspect of the skin, namely
to "suffer" a little longer from the more intense side effects
the epidermis, is what patients first see when looking in the
of the treatment rather than not resolve the problem of the
mirror, and beneficial changes in the epidermis can be
wrinkles. Patient education is, therefore, extremely impor-
achieved in grade I wrinkles with one or two passes with
tant to manage realistic patient expectations.
the fractional Er:YAG laser and the short pulse programme,
Fractional resurfacing with Er:YAG laser with low
with little thermal damage in the dermis accelerating the
incident doses and few passes for wrinkle treatment will
repair process. The medium pulse programme with more
obviously require more than one treatment session to
passes is required for more noticeable grade II wrinkles, to
enhance the condition of moderate to severely photo-aged
deposit more heat into the dermis and start neocollagenesis.
skin. However, each subsequent treatment session at the
For much more established grade III wrinkles, however, the
same parameters will not go any further than the previous
Fig. 4 Caucasian woman, 48years old, skin phototype II, (a)before and (b) 1 week afterfractional resurfacing of theupper lip. Tissue has healed afterskin ablation, with clear im-provement of the wrinkles;however, clear signs of herpessimplex infection are observed.
c Aspect at 2 months aftertreatment. Herpetic lesion hashealed without any scarring, butsome lesion-related residual er-ythema is still present. Wrinklesare significantly better
session and will fail to trigger the essential dermal wound
such as frowning, looking surprised, laughing, looking
healing processes, which are absolutely essential to achieve
angry, and so on. In this way, wrinkles and lines not
a better in-depth skin condition and for the elimination of
obviously apparent can be seen, thus helping the clinician
lines and wrinkles. In contrast, as seen in this study, with
to determine the true aspect of the wrinkles on a patient-by-
only one treatment at high energies and multiple passes, the
patient basis.
results were evident even in grade III wrinkles. One
Our study showed that pain was not a major problem
particularly interesting advantage is that, although the
during treatment, and there were no side effects. The
dermis is affected and the epidermis eliminated, tissue
absence of complications, except in the one patient who
healing is achieved quite quickly. From 5 to 7 days after
presented with hyperpigmentation, can be used as an
one single treatment, the skin was free of fine scabs and had
argument to recommend a second session of treatment for
a rejuvenated aspect with minimized erythema. This is easy
those patients whose expectations have not been met. Once
to mask with cosmetics, and patients are ready to return to
again, the importance of managing realistic patient expect-
their business or social life in a very short time.
ations is clear. "Top-up" sessions at subsequent intervals
Interviews with patients have shown that compliance
will also thus be well-accepted.
with a laser resurfacing protocol is better when only a
The fractional ablative Er:YAG laser device used in this
single treatment is carried out. Moreover, the increased SI
study has other possible applications in various skin
2 months after treatment in patients treated with the higher
disorders and aesthetic conditions, in relation to ageing
energy density of the long pulse programme and eight
and cicatricial pathologies. The combination of fractional
passes matched the expected results better.
resurfacing with, for example, an IR wavelength hand-
Previous observations extracted from patients treated by
piece, used before ablative fractional resurfacing with the
us with the same device (data not published) and a number
Er:YAG hand-piece, can heat the dermis, possibly adding
of treatment sessions with a more conservative pulse
extra value to improve the final results. The instigation of
programme and fewer laser passes did not show better
an appropriate adjunctive regimen of epidermal care might
results than those achieved with only one treatment with the
also help improve results even more, as might
technique described above. In our experience, often when
adjunctive phototherapy with light-emitting diodes (LEDs)
patients are interviewed before treatment, they do not wish
of appropriate wavelengths.
to undergo various sessions of treatment, and, even when
The histological findings 2 months after treatment
they agree to a multiple treatment regimen, compliance
showed a better collagen appearance, more evident in those
with the protocol can be less than perfect. The feasibility
patients treated with high energy levels and multiple passes.
and efficacy of our treatment protocol are justified by the
Improvement in the dermal architecture and organization
fact that no patient reported any complications and that all
seen in the histology 2 months after treatment were very
completed both the assessment points.
well correlated with the better external gross aspect of the
Clinical improvements obtained with non-ablative
area treated, which was clearly the reason behind the high
lasers are, in general, modest at best [So far, devices
SI of 83% as reported by patients at the 2-month
for skin rejuvenation associated with the use of all types of
assessment point.
non-ablative rejuvenation treatments provide excellentdermal histology and good collagen remodelling. Howev-er, these achievements are not always echoed in enough
epidermal rejuvenation and patient satisfaction –and, moreover, the long treatment regimens associated
Fractional resurfacing with Er:YAG laser in only one
with non-ablative methods also cause problems with
treatment session can achieve effective skin rejuvenation,
patient compliance.
with effects on both the epidermis and dermis. If the
In this study, the results were satisfactory in all those
treatment programme chosen is the long pulse mode, at
patients presenting with grade I and grade II wrinkles,
1,400 mJ total energy per pulse, and eight passes are carried
treated in one session with the short and long pulse
out, the results obtained, as illustrated in our study, can be
programme, respectively, but degree II wrinkles appeared
highly efficacious and can be clinically and histologically
to benefit less from the medium pulse programme. This
demonstrated. The treatment programme can be accurately
could be because degree II wrinkles correspond to an
correlated, according to the degree of the signs of photo-
intermediate phase of dermal tissue deterioration, and visual
aged skin intended for rejuvenation. No complications were
diagnosis fails to be totally accurate. Clinicians should be
noted, except for one case of slight hyperpigmentation in a
aware that, when examining patients for wrinkle diagnosis
woman with phototype IV skin. Side effects, such as pain,
and allocation of pulse programme treatment, patients
discomfort, fine scabbing, oedema and erythema, are well
should be asked to accentuate a range of facial expressions,
tolerated and accepted by patients. The side effects can
be very well controlled, so, if necessary, extra treatment
European Academy of Dermatology and Venereology Congress,
sessions can be carried out.
16–20 May 2007, Vienna, Austria
6. Lee MW (2002) Combination visible and infrared lasers for skin
The authors declare no financial or other
rejuvenation. Semin Cutan Med Surg 21:288–300
interest in the companies and/or equipment mentioned in this study.
7. Lee MW (2003) Combination 532-nm and 1064-nm lasers for
The report given in this study is registered in the academic activities of
noninvasive rejuvenation and toning. Arch Dermatol 139:1265–
the Fundacion Antoni de Gimbernat, 2006–2007.
8. Tanzi EL, Williams CM, Alster TS (2003) Treatment of facial
rhytides with a nonablative 1,450-nm diode laser: a controlled andhistologic study. Dermatol Surg 29:124–128
9. Menaker GM, Wrone DA, Williams RM, Moy RL (1999)
Treatment of facial rhytides with a nonablative laser: a clinical
1. Gold MH (2007) Fractional technology: a review and clinical
and histological study. Dermatol Surg 25:440–444
approaches. J Drugs Dermatol 6:849–852
10. Goldberg DJ (1999) Non-ablative subsurface remodeling: clinical
2. Bitter PH (2000) Noninvasive rejuvenation of photoaged skin
and histological evaluation of a 1320 nm Nd:YAG laser. J Cutan
using serial full-face intense pulsed light treatments. Dermatol
Laser Ther 1:153–157
Surg 26:835–843
11. Goldberg DJ (2000) Full-face nonablative dermal remodeling with
3. Trelles MA, Mordon S, Benítez V, Levy JL (2001) Er:YAG laser
a 1320 nm Nd:YAG laser. Dermatol Surg 26:915–918
resurfacing using combined ablation and coagulation modes.
12. Trelles MA, Allones I, Luna R (2001) Facial rejuvenation with a
Dermatol Surg 27:727–734
nonablative 1320 nm Nd:YAG laser: a preliminary clinical and
4. Miller LD (1997) The erbium laser gains a role in cosmetic
histological evaluation. Dermatol Surg 27:111–116
surgery. Biophoton Int May/June 38–42
13. Trelles MA, Allones I, Velez M (2003) Nonablative facial skin
5. Trelles MA (2007) Red light-emitting diode (LED) therapy assisted
photorejuvenation with an intense pulsed light system and
healing improves results of facial skin fractional resurfacing. 16th
adjunctive epidermal care. Lasers Med Sci 18:104–111
Source: http://www.harmony.cl/files/PIXEL.pdf
Volume 11 Number 2 February 2015 Pages 321–666 Molecular BioSystems Interfacing chemical biology with the -omic sciences and systems biology Tong Wang, Gong Zhang et al.Length-dependent translation initiation benefi ts the functional proteome of human cells Length-dependent translation initiation benefitsthe functional proteome of human cells†
Traducido del Texto "Endodontics" de Arnaldo Castellucci MD, DDS Vol. 1. Primera Ed. 2.004 Traducción: Dr. Carlos Heilborn. Odontólogo. Especialista en Endodoncia. Asunción - Paraguay EL SÍNDROME DEL DIENTE FISURADO Uziel Blumenkranz S. DDS Si uno considera las varias quejas de los pacientes con diferentes formas de patología pulpar, por ej. sensibilidad al frío en la hiperemia o sensibilidad al calor en las pulpitis; o de patología peri apical, por ej. dolor desencadenado por presión en una periodontitis o absceso, uno puede concluir que éstos no pueden coexistir en el mismo diente. Mientras el paciente puede manifestar que el diente es sensible al calor, frío y presión, esto se debe generalmente a la condensación de síntomas de odontalgias previas. Sin embargo, existe un caso en el cual estos tres síntomas pueden originarse y coexistir en un mismo diente. Esto se conoce como el "síndrome del diente fisurado". Introducción Hasta el año 1.964 se han sugerido muchos nombres para esta condición. Pero fue Cameron quien introdujo el término "síndrome del diente fisurado", agregando que "el factor más importante para el diagnóstico del diente fisurado es el conocimiento de que estas fisuras suceden". Aunque se han escrito muchos artículos sobre este tema desde entonces, muchos pacientes con este síndrome están sin diagnóstico. Además existe una confusión en la literatura dental al respecto de los dientes diagnosticados con el "síndrome del diente fisurado" y aquellos fracturados como consecuencia de accidentes de procedimientos. Las fracturas de la última categoría han sido denominadas Fracturas Apicales Inducidas por Williams y fracturas radiculares verticales, por otros. Mientras que en ambos casos el la consecuencia en el diente puede ser la misma, la etiología es diferente. También es un hecho que mientras que la profesión dental se valga principalmente de las evaluaciones radiográficas, este síndrome no puede ser fácilmente identificado. Las fisuras se producen de mesial a distal, donde las películas radiográficas son incapaces de capturarlas. Por tanto, más y más dientes serán víctimas del "síndrome del diente fisurado". Aún así, si se detectan pueden ser salvados. Los dientes fisurados son muy difíciles de diagnosticar, especialmente si el dentista no los está buscando. En muchos casos, debido a la ignorancia por parte del dentista, el paciente es tildado de "paranoico", y es enviado a su casa con una prescripción de tranquilizantes. Es notable que en su estudio Cameron reportó que un paciente aquejado del síndrome del diente fisurado estaba siendo medicado con Tegretol debido a una posible neuralgia trigeminal y para otro se estaba considerando cirugía cerebral. Los dientes fisurados son un estadio intermedio de una serie de eventos que, si no se reconocen y no se tratan, culminarán con la extracción del diente. El diagnóstico y tratamiento precoces a menudo pueden prevenir molestias innecesarias y tratamientos más invasivos. Definición El "Síndrome del Diente Fisurado" se caracteriza por una fractura incompleta de un diente posterior con pulpa vital, la cual incluye dentina y posiblemente la pulpa dental. En un intento de expandir el dominio del síndrome, deben incluirse también en esta definición los dientes fisurados con necrosis pulpar y/o abscesos dentoalveolares. Un diente se considera "fisurado" cuando los potenciales segmentos de la fractura se mantienen intactos por una porción del diente a través del cual la fractura aún no se ha extendido. La "fisura" se refiere a una disrupción o interrupción de la continuidad de la







