Microsoft word - terb ar2008 final.doc
The Vermont
Tobacco Evaluation
& Review Board
Annual Report
the Governor
the General Assembly
January 2008
TABLE OF CONTENTS
EXECUTIVE SUMMARY
I. VERMONT TOBACCO CONTROL PROGRAM OVERVIEW
Program Goals Program Components and Structure Program Funds
II. EVALUATION OF THE COMPREHENSIVE PROGRAM
Timeline of Expected Program Outcomes and Statistical Note Awareness of Program Services Attitudes toward Smoking Youth Smoking Prevalence Adult Smoking Prevalence Exposure to Secondhand Smoke
III. EVALUATION OF PROGRAM COMPONENTS
Tobacco-Free Community Coalitions School-based Tobacco Use Prevention Program Smoking Cessation Services Statewide Training of Health Care Providers Media and Public Education Enforcement of Laws Banning Tobacco Sales to Minors
IV. ROLE OF THE BOARD
Responsibilities Board Actions in 2007
V. BOARD RECOMMENDATIONS
Legislative & Other Policy Recommendations Memo from the Board Chair FY2009 Program and Budget Overview
VI. FINANCIAL REPORTS
Vermont Tobacco Evaluation & Review Board Department of Health Department of Education Department of Liquor Control
APPENDICES
1. Board Members and Terms 2. CDC Tobacco Control Program Budget Recommendation for Vermont 3. Vermont Smoking Rates 4. Vermont Kids Against Tobacco & Our Voices Exposed Grants, FY2008
EXHIBITS & APPENDICES
Structure of Vermont Tobacco Control Program
Appropriations for the Tobacco Control Program, FY2001-FY2004
Appropriations for the Tobacco Control Program, FY2005-FY2008
Timeline of Expected Program Outcomes
Awareness of Assistance to Help Quit Smoking
Perceived Eligibility for Free or Reduced Cost NRT by Insurance Type
Smoking Prevalence among Vermont Youth by Grade, 1993 – 2007
Smoking Rates: Vermont, Neighboring States and U.S.
Percentage of Smokers Who Seriously Tried to Quit in the Last 12 months
Current Smokers Who Have Never Used NRT, Zyban or Chantix
Current Smokers Recommended a Specific Medicine or Program
Percentage of Vermont Smokers with Smoke-Free Policies in the Home
Percentage of Vermonters with Smoke-Free Policies for Cars
Community Coalition Activities by Program Goal Addressed
Community Coalition Grants by County, FY2008
School-based Tobacco Grants by County, FY2008
Implementation of Research-based Tobacco Use Prevention Curricula
Ready, Set…STOP Grants to Hospitals, FY 2008
New Clients Served by Quit Line, Ready, Set.STOP and QuitNet
Reach of Cessation Services
Rates of Completion of Follow-up Contacts with Counseling Clients
Quit Rates for Current Smokers Counseled
Fax referrals from health care providers to cessation services
Vermont State Dental Society Trainings
Calls to the Quit Line and Ready, Set…STOP
Department of Liquor Control Tobacco Compliance Rates
Retail Clerks Training and Tobacco Compliance Checks
Board's FY2009 Program & Budget Recommendation
Financial Reports, First Half of FY2008:
Tobacco Evaluation and Review Board
Department of Health
Department of Liquor Control
Department of Education
Vermont Tobacco Evaluation & Review Board: Members
CDC: Vermont Budget Recommendation
Smoking Rates in Vermont, By Age and Specific Populations
Vermont Kids Against Tobacco and Over Voices Exposed, FY2008 grants
Vermont Tobacco Evaluation & Review Board
Eighth Annual Report to the Governor and General Assembly, January 2008
EXECUTIVE SUMMARY
MAJOR FINDINGS & RECOMMENDATIONS
The Good News
Adult Smoking Rate
The overall smoking rate among all adults (age 18 and older) dropped to 18% in 2006, the first
significant decrease since 2000.
-
2006 Behavioral Risk Factor Surveillance System
Youth Smoking Rate
The majority of students have never smoked a whole cigarette. In 2007, 29% of students reported
having smoked a whole cigarette, down from 57% in 1997.
-
2007 Youth Risk Behavior Survey
Secondhand Smoke Exposure
89% of households with children prohibit smoking in the home in 2006
. These voluntary
prohibitions on smoking may indicate rising public awareness of the dangers of secondhand
smoke as well as changing social norms concerning exposure to secondhand smoke.
The Bad News
Smoking rates among specific populations of Vermonters are higher than the overall adult smoking rate of 18%:
20% of pregnant women smoke.
30% of Vermonters living below 125% of the Federal Poverty Limit (FPL) smoke.
27% of Vermonters between the ages of 18-24 smoke.
44% of Vermonters with moderate or severe depression smoke.
Vermont is not likely to reach the state's 2010 goal of reducing the adult smoking rate to 11% with current efforts.
The Board's Budget Recommendation
The Vermont Tobacco Evaluation and Review Board recommends an increase of $3.2 million for a total of $8.4 million in tobacco control program funds for FY2009. This increase will address areas - in particular adult smoking cessation – that need to be enhanced in order to achieve the state's long-term objectives. Investment in the state's comprehensive tobacco control program is critical to improving the health and reducing health care costs of all Vermonters. A concise overview of the specific recommendations is outlined on the next page.
This report details the significant progress that the statewide program has made, particularly in
reducing the youth smoking rate and exposure to secondhand smoke. It also documents
positive
trends since 2001:
The majority of healthcare professionals talk to their patients about smoking.
Media campaigns have increased awareness of smoking cessation services.
More smokers are using nicotine replacement therapy in their quit attempts.
Most Vermonters are aware of local programs aimed to prevent youth smoking.
This report also discusses
four areas of concern:
Most publicly insured and uninsured Vermonters do not know or are unsure if they
are eligible for free nicotine replacement therapy.
Although the majority of healthcare professionals talk to their patients about
smoking, most do not refer their patients to a smoking cessation program or
medication.
Although the number of smokers enrolled in the hospital-based Ready, Set…STOP
program and Quitline is increasing, total enrollment is only a small percentage of
Vermonters who tried to quit smoking.
The prevalence of quit attempts, of intentions to quit and, of confidence in quitting
among adult smokers is not increasing.
The Board's Budget Recommendation: Program Enhancements
The Tobacco Evaluation and Review Board recommends a $3.2 million increase for a total of $8.4 million in FY2009 to:
Increase availability of free nicotine replacement therapy through the Quit Line and physicians' offices.
Work with health care providers to increase the use of systems to identify and counsel smokers and to connect them to smoking cessation resources.
Increase media efforts to encourage and motivate quit attempts among adults.
Tailor smoking cessation programs to populations with higher smoking rates.
Expand community tobacco coalitions to areas of the state that do not have access to coalition services; increase leadership and communication skills training.
Expand media efforts to prevent youth from smoking.
Explore new ways to reach smokers to encourage quit attempts and to seek treatment.
Increase the number of educators licensed to teach health education.
Expand enforcement of tobacco-related laws.
For more details, see Section V of this report.
The principal focus of this report is the results of the independent evaluation of Vermont's
Tobacco Control Program. RTI International, who evaluates policy and program outcomes for
Vermont and numerous other states, stated in 2006 and 2007:
"Youth smoking rates have decreased significantly in Vermont and the rate of decline has been
considerably greater than the rate of the rest of the U.S."
"While the [overall] adult smoking rate in Vermont [18%] remains lower than the average for the
rest of the United States [20.8%], the rate of decline is not significantly different between
Vermont and the rest of the United States
."
VERMONT'S COMPREHENSIVE PROGRAM
The Vermont Tobacco Control Program was created in FY2001 with the ambitious goal of
cutting smoking rates in half in 10 years. The strategy to reach that goal was to implement a
research-based, comprehensive program that includes components that the Centers for Disease
Control and Prevention (CDC) identified for successful statewide programs.
The seven components of the Vermont Tobacco Control Program are:
1. Tobacco-free community coalitions 2. School-based tobacco use prevention program 3. Services to help smokers quit 4. Statewide training for health care providers 5. Media and public education 6. Enforcement of laws to prevent tobacco sales to minors 7. Evaluation of outcomes and feedback to improve programs
The program is funded with Master Settlement Agreement (MSA) funds appropriated to the following:
Department of Health: community coalitions, smoking cessation services, statewide provider education, surveillance, media, and public education
Department of Education: school-based tobacco use prevention program
Department of Liquor Control: enforcement programs to educate retailers about tobacco sales laws and conduct compliance checks to assess adherence to the laws
Tobacco Evaluation & Review Board: oversees the independent evaluation of the program, approves media campaigns, reviews applications for coalition grants, holds annual public meetings, provides annual recommendations for program funding, reviews program components and recommends strategies for increased collaboration
EVALUATION OF STATEWIDE PROGRAM
At the outset of the program, a timeline was developed to provide benchmarks for evaluating
progress toward the 2010 goals. Vermont's comprehensive tobacco control program was
designed to have all components of the program act synergistically to effect changes in
awareness, attitudes, and behaviors that lead to a 50% reduction in smoking by 2010.
The independent evaluation involves two types of tasks. The first focuses on the statewide program to determine if program outcomes - the changes in awareness, attitudes, and behaviors - are occurring as expected and as a result of program activities. The second focuses on each of the seven program components to assess if they are being implemented as planned and to identify strengths and areas for improvement.
EVALUATION OF PROGRAM COMPONENTS This report provides detailed information regarding the activities conducted and services
provided through the tobacco control program. The report also includes evaluation data linking
program activities with changes in attitudes and behaviors.
The standards against which the program components are assessed are the measurable objectives
listed in the
Vermont 2008 & 2009 Tobacco Control Work Plan. Listed below are a few of the
findings, detailed in this report, from the evaluation of each of the program components.
Community Tobacco Coalitions
In FY2007, coalitions conducted 683 activities. 42% of the activities focused on youth prevention, 31% on smoking cessation and 19% on reduction to secondhand smoke exposure.
76% of Vermont smokers reported awareness of programs that help young people avoid smoking.
School-based Programs
94% of schools had a tobacco-free policy in place in FY2007.
61% of schools provided students with evidence-based tobacco prevention curricula in FY2007.
Services to Help Smokers Quit
New clients served by the Ready, Set…STOP
smoking cessation program at Vermont's hospitals totaled 1,936 in FY2007, an increase of 30% over the previous year.
The percentage of callers to the Vermont Quit Line increased by 4% in FY2007 from FY2006.
Media and Public Education
91% of all Vermonters reported awareness of at least one quit smoking media message in 2006.
86% of Vermont smokers reported a quit smoking ad made them think about whether or not they should smoke in 2006.
Enforcement of Laws to Prevent Tobacco Sales to Minors
In calendar year 2007, the Department of Liquor Control (DLC) completed 1,512 compliance checks.
The rate of compliance (i.e. did not sell to minors) among tobacco licensees was 87% in calendar year 2007 and 88% in FY2007, above the federal requirement of 80% compliance but below the required rate of 90% compliance in Vermont.
I. VERMONT TOBACCO CONTROL PROGRAM OVERVIEW
PROGRAM GOALS
The goal of the Vermont Tobacco Control Program is to decrease smoking among adults and
youth by 50% between 2000 and 2010. The long-term outcomes expected of the program are
therefore the following:
• To reduce the prevalence of smoking among Vermont adults from a rate of 22% in 2000
to a rate of 11% in 2010
• To reduce the prevalence of smoking among Vermont youth from a rate of 31% in 1999
to a rate of 15% in 2010
• To reduce the exposure of all Vermonters to secondhand smoke
Each component of the program is designed to address one or more of the following objectives:
• To prevent youth from smoking • To help smokers quit • To reduce exposure to secondhand smoke, especially among children
PROGRAM COMPONENTS AND STRUCTURE
The strategies to reach these goals were detailed in the
Vermont Best Practices to Cut Smoking
Rates in Half by 2010, published by the Vermont Department of Health in January 2000. It was
based on the Centers for Disease Control and Prevention's (CDC)
Best Practices for Tobacco
Control that calls for a comprehensive, research-based program that includes multiple
components.
The Vermont Tobacco Control Program includes the following seven components:
1. Tobacco-free community coalitions 2. School-based tobacco use prevention program 3. Smoking cessation services 4. Statewide training programs for health care providers 5. Media and public education 6. Enforcement of laws to prevent tobacco sales to minors 7. Evaluation
The strategy of the program is to integrate these components at the statewide and the local level in order to reinforce the activities and messages of each and to achieve synergism. When the Legislature established the Tobacco Control Program effective FY2001, it appropriated funds for each of the above components. The four entities charged with implementing and evaluating the program are the Departments of Health, Education, Liquor Control, and the Vermont Tobacco Evaluation & Review Board. See Exhibit 1 for the overview of the structure of the Vermont Tobacco Control Program. If a department contracts the program out, the contractor is identified in parentheses next to the program.
Structure of Vermont Tobacco Control Program
DEPARTMENT OF HEALTH
Tobacco-Free Community Coalitions
19 community coalition grantees
Cessation Services to Help Smokers Quit
Vermont Quit Line: free telephone counseling (American Cancer Society)
Ready, Set.STOP: free group & individual counseling at 13 hospitals (Fletcher Allen Health Care)
Quit Net: free interactive, secure website that provides individual smoking cessation plans, information about quitting and Vermont smoking cessation services (Healthways, Inc)
Nicotine Replacement Therapies (NRT): free or discounted NRT shipped directly to smokers enrolled in the Quit Line or Ready, Set…STOP program
Not-On-Tobacco Program: teen smoking cessation (American Lung Association of Vermont).
Health care provider training programs (John Snow International)
Media and Public Education
Campaigns: youth prevention, promotion of cessation services & reducing exposure to secondhand smoke (Kelliher Samets Volk)
Youth Empowerment
Vermont Kids Against Tobacco and Our Voices Exposed: middle & high school anti-tobacco groups, mini-grants funded by Centers for Disease Control and Prevention
Surveillance and Evaluation
Surveys: conduct general health surveys and tobacco-specific surveys of youth and adults
Program data: report by each grantee and contractor
DEPARTMENT OF EDUCATION
Tobacco Use Prevention Program
Grant allocations available to supervisory unions for part-time coordinator to promote research-based curricula, model tobacco-free policy and link community and family to tobacco prevention initiatives
Governor's Youth Leadership Conference: tobacco track
Program data: report by each tobacco use prevention coordinator
DEPARTMENT OF LIQUOR CONTROL
Retailer Training and Compliance Checks
Training: seminars for retail managers and clerks
Compliance: checks on randomly selected tobacco licensees
Program data: training and compliance databases to monitor results
TOBACCO EVALUATION & REVIEW BOARD
Independent evaluation: selects contractor and oversees work
Annual report: provides program progress and areas for improvement
Budget: makes annual recommendation to Governor and Legislature
Media: approves all campaigns
Public meetings: implements annual meetings for input on program and budget
Community coalitions: reviews grant applications and submits funding recommendations to Commissioner of Health
Program work plan: develops program strategies and objectives bi-annually with the three departments
PROGRAM FUNDS
Annual State Funds
The principal source of funding for the Vermont Tobacco Control Program is from a portion of
the Master Settlement Agreement (MSA) payments made annually to the state by the major
tobacco companies in settlement of the multi-state civil law suit. Vermont has received MSA
payments of approximately $25 million in most years since FY2000. $17.25 million has been
appropriated each year to the Health Access Trust Fund for Medicaid and Vermont Health
Access Plan (VHAP).
Vermont's FY2008 tobacco control program budget is $5.2 million (14% of anticipated FY2008
MSA payment). See exhibits 2a and 2b for line item appropriations. In October 2007, the Centers
for Disease Control and Prevention (CDC) recommended that Vermont spend double the current
budget - $10.4 million – on comprehensive tobacco control.1 Research shows that the more states
spend on comprehensive tobacco control programs, the greater the reduction in smoking. The
longer states invest in such programs, the greater and faster the impact. States that invest more
fully in comprehensive tobacco control programs have seen cigarette sales drop more than twice
as much as in the United States as a whole, and smoking prevalence among adults and youth has
declined faster as spending for tobacco control programs has increased. A recent peer-reviewed
report concluded that state tobacco control expenditures are independently associated with
overall reductions in adult smoking prevalence.2
External Funds
In addition to state funds, the Vermont Department of Health (VDH) receives a grant of
approximately $1 million annually from the CDC for tobacco control. This is largely devoted to
personnel and overhead, with some funds for special initiatives. For example, VDH used CDC
funding to develop a strategy to address tobacco-related health disparities among low income
and mentally ill populations. VDH is applying for a competitive grant from the Substance Abuse
and Mental Health Services Administration (SAMHSA) to enhance efforts to address tobacco
use among persons with co-occurring mental health and substance abuse issues in FY2009.
Long-term Funding
In 1999, the Legislature and Governor created the Tobacco Task Force and charged it with
developing a comprehensive plan for use of the MSA funds. The task force held hearings
throughout the state to ascertain how Vermonters wanted to spend the annual MSA payments.
The task force recommended the following annual allocation of MSA funds:
33% - Tobacco Control Program
33% - Health Access Trust Fund
33% - Tobacco Trust Fund (for a sustainable source of funds for the tobacco
control program that is not dependent on the tobacco industry)
The first MSA payment of $10.2 million was made in FY1999 and was appropriated to the Tobacco Trust Fund. An additional $6 million was appropriated to it in FY2000 and $3 million in FY2001. The Tobacco Trust Fund balance on June 30, 2001 was $21.6 million. No additional appropriation has been made to the fund since then, although the fund accrues investment earnings and had a final balance of $30.9 million at the end of FY2007. 1Best Practices for Comprehensive Tobacco Control Programs, U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, October 2007. 2 Matthew C. Farrelly, PhD, The Impact of Tobacco Control Programs on Adult Smoking, American Journal of Public Health, Volume 98, No. 2, published ahead of print, Jan. 2, 2008.
Appropriations for the Tobacco Control Program, FY2001-FY2004
July 2000 – June 2001
July 2001 – June 2002
July 2002 – June 2003
July 2003 – June 2004
TOBACCO CONTROL PROGRAM
FY 2001*
FY 2004***
Original Adjusted**
DEPARTMENT OF HEALTH
Community Coalitions
Media & Public Education
Cessation Services
Statewide Provider Education
Evaluation: Surveys + Ind. Evaluation
Department of Health Total
4,830,000
1,975,161
3,234,724
3,887,804
DEPARTMENT OF EDUCATION
Grants to schools for prevention
1,200,000*
DEPT OF LIQUOR CONTROL
Retailer training & compliance checks
TOBACCO EVALUATION BOARD
PROGRAM TOTAL
$6,464,000 $5,534,000
$3,334,161
$4,532,677
$5,211,259
* FYO1: $412,500 was cut from the FY01 appropriation for evaluation in Budget Adjustment due to the reduction in the MSA payment
(A penalty for the delay in Vermont's passage of the Non-Participating Manufacturers' (NPM) provision). This delayed the start of the independent evaluation contract until February 2002. In addition, some positions were not yet approved for the Department of Education tobacco prevention program.
** FY02: Rescissions for budget deficit prevention required the Department of Health to shift all of their FY02 grants and contracts from a calendar year to the state fiscal year, and to absorb some reductions in program funding. ***FY04: $500,000 of the FY04 appropriation is one-time General Funds; the remaining amount in FY04 and all other tobacco control program funds
Appropriations for the Tobacco Control Program, FY2005 – FY 2008
July 2004 – June 2005
July 2005 – June 2006
July 2006 – June 2007
July 2007 – June 2008
TOBACCO CONTROL PROGRAM
DEPARTMENT OF HEALTH
Community Coalitions
Media & Public Education
Cessation Services
Statewide Provider Education
Evaluation: Surveys + Ind. Evaluation
Department of Health Total
3,399,677
3,481,423
+up to $500,000 #
DEPARTMENT OF EDUCATION
Grants to schools for prevention
DEPT OF LIQUOR CONTROL
Retailer training & compliance checks
TOBACCO EVALUATION BOARD
PROGRAM TOTAL
$4,668,657
$4,855,193
$5,114,371
$5,224,947
**** FY07 and FY08: Department of Health total includes $543,696 (FY07) and $1,059,409 (FY 08) from Global Commitment Funds. # FY08: If Strategic Contribution Fund (SCF) is greater than $13 million but less than $13.5 million, then up to $500,000 shall be
appropriated to the Department of Health for tobacco programs. If SCF is $13.5 million or greater in FY08, then $500,000 shall be appropriated to the Department of Health for tobacco programs.
II. EVALUATION OF THE COMPREHENSIVE PROGRAM
TIMELINE OF EXPECTED PROGRAM OUTCOMES
The
Timeline of Expected Program Outcomes was established for a comprehensive tobacco
control program in Vermont before the program was funded (Exhibit 3). It was based on the
outcomes achieved by comprehensive tobacco control programs in other states, and was
reviewed by the board's Evaluation Committee after the Centers for Disease Control and
Prevention (CDC) published the
Introduction to Program Evaluation for Comprehensive
Tobacco Control Programs in November 2001.
While it is very difficult to predict exactly when
each step will occur, the timeline was developed to provide benchmarks for evaluating progress
toward the 2010 goals.
Exhibit 3
Program Outcomes
The program evaluation does not link to individual program components with an outcome. For
example, one would not expect that reductions in youth smoking are solely the result of
school-based programs. Rather, the comprehensive tobacco control program has been designed
to have all of the components of the program act synergistically to produce the expected
outcomes.
To assess the impact of the entire program, the independent evaluation has been tracking results
for each of the outcomes shown in the timeline:
Awareness of program services and messages
Attitudes toward smoking
Consumption of cigarettes
Prevalence of smoking among youth
Prevalence of smoking among adults
Exposure to secondhand smoke among all Vermonters
AWARENESS OF PROGRAM SERVICES IS MIXED
According to the timeline
, by 2002 all of the component programs should have been fully
implemented, and Vermonters should have been aware of the program by 2003. Between 2001
and 2002, awareness of program services and messages rose sharply and has since leveled off.
This is true whether examining the Vermont Adult Tobacco Survey (ATS) results for all
Vermonters or for particular target populations. Reported awareness has consistently been
highest for local programs to help people quit smoking, followed by awareness of programs to
help young people avoid smoking and programs that discourage people from smoking around
children.
The ATS asks participants if there are programs in their area that help adults quit smoking. As
shown in Exhibit 4, the majority of Vermont smokers reported awareness of cessation programs
in their area (87.5%) in 2006. This is a significant increase from 2001 (60.8%).
EXHIBIT 4: Awareness of Assistance to Help Quit Smoking among Current Smokers (VT ATS)
Cessation programsa
a significant linear trend
The level of awareness differs very little by education levels or income levels. This is important because, while smokers are much more likely to be of lower income and education levels, the awareness of smoking cessation programs is equally high among smokers across education levels. This suggests that the program has done a good job of reaching all smokers with information about services.
Overall, the percentage of Vermont smokers who perceive "very easy" access to all cessation resources has increased between 2001 and 2006. The percentage of Vermont smokers who perceive access to group cessation programs to "very easy" has continually increased since 2001. In contrast, the trend in the percentage of smokers who reported "very easy access" to the Vermont Quit Line, to information and booklets about quitting has leveled off over time. The percentage of current smokers with public insurance (Medicaid, VHAP, Medicare and Ladies First) who perceive they are eligible for free or reduced cost NRT is significantly higher than the percentage of those who are not insured or have other insurance (Exhibit 5). However, among all groups, the percentage of current smokers who think they are eligible for free or reduced cost NRT is low. In addition, the percentage of current smokers who reported that they
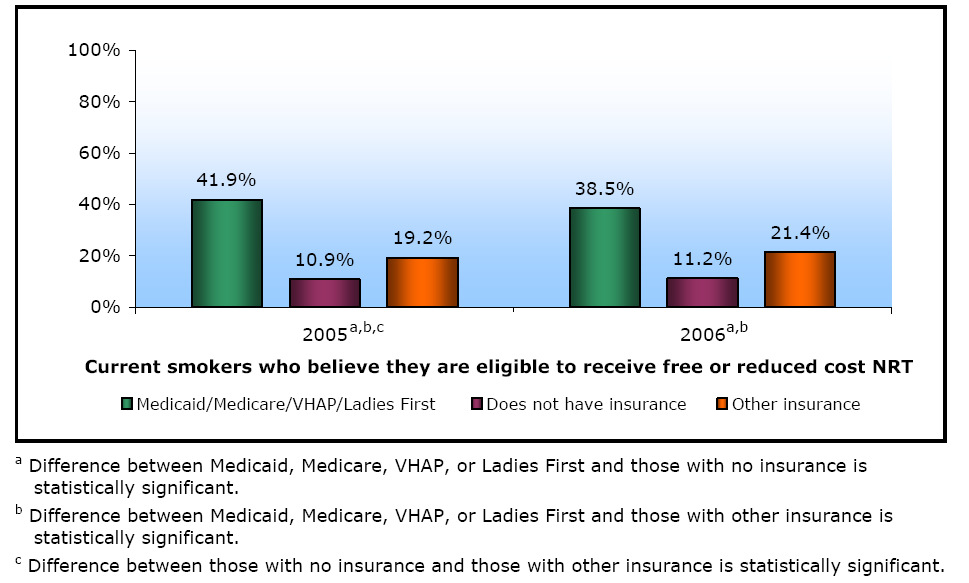
did not know or were not sure about their eligibility for free or reduced cost nicotine replacement therapy (NRT) increased significantly from 2005 to 2006. These results suggest a need to educate smokers about their eligibility and promote existing programs among eligible smokers. EXHIBIT 5: Perceived Eligibility to Receive Free or Reduced Cost NRT by Insurance Type (current smokers), 2005-2006
ATTITUDES TOWARD SMOKING MAY BE SOFTENING
According to the timeline, Vermonters' attitudes toward tobacco should have been significantly
more negative by 2004. In fact, changes in those attitudes were apparent by 2002. However,
ATS data suggest that negative attitudes toward tobacco seem to have softened over time. There
appears to be a small but grower number of people with permissive, or at least indifferent,
attitudes toward adult smoking.
Attitudes among Youth
According to the 2006 Youth Health Survey (YHS), 43% of middle school students believe that
a significant proportion of high school students currently smoke cigarettes. Although this is a
significant improvement from 2000 when 62% of middle school students believed most high
school students smoke, it is a decline from the 37% who believed it in 2004. 74% of students
believe smoking does not make you look cool. The majority (63%) of students believe that
smoking for a year or two is not safe and 78% of students are aware that secondhand smoke is
unhealthy.
Attitudes among Adults
According to the ATS, the percentage of Vermonters who said that it is okay for adults to smoke
as much as they want increased from 7.2% in 2003 to 12.3% in 2006. In addition, the percentage
of smokers who think that most people in their community think it okay for adults "to smoke as
much as [they] want" increased between 2001 and 2006, although the upward trend has leveled
off in 2005 and 2006.
YOUTH SMOKING PREVALENCE VIRTUALLY AT GOAL
Vermont set a goal of reducing the prevalence of youth smoking from 31% in 1999 to 15% in
2010. The percentage of Vermont students in grades 8 through 12 who reported, in the Youth
Risk Behavior Survey (YRBS), smoking on at least one of the past 30 days fell from 31% in
1999 to 16% in 2005 and remained at 16% in 2007 (Exhibit 6). This is a decline of 48% since
the tobacco control program began. Vermont has virtually met the goal of a 50% reduction in
youth smoking, in just five years rather than the anticipated 10 years. According to RTI, youth
smoking rates have decreased significantly in Vermont and the rate of decline has been
considerably greater than the rate of the rest of the U.S.
EXHIBIT 6: Smoking Prevalence among Vermont Youth by Grade, 1993 – 2007 (VT YRBS)
OVERALL ADULT SMOKING PREVALENCE DECLINES
From 2003 to 2005, the overall smoking rate among all adults (age 18 and older) ranged from
19.3% to 20%. The adult smoking rate dropped to 18% in 2006, the first significant decrease
since the tobacco control began. According to RTI, however, there is no evidence that the rate of
decline in Vermont is greater than in the rest of the country (Exhibit 7). Vermont is not likely to
make the goal of reducing the adult smoking rate to 11% by 2010 with current efforts.
Some populations experience a disproportionate health and economic burden from tobacco use,
according to the Centers for Disease Control and Prevention. In Vermont, the smoking rate
among those living in poverty is 30%, and 40% of clients of mental health and substance abuse
clinics smoke. Vermont has one of the highest smoking rates (20%) among pregnant woman in
the nation. Additional investments are needed to address those disparately impacted by tobacco
use and to increase adult smoking cessation rates in order to meet the state's 2010 goal.
EXHIBIT 7: Current Smoking in Vermont, Neighboring States and the Rest of the United States (BRFSS)
Quitting Smoking: Confidence, Attempts and Methods
The percentage of Vermont current smokers who are very confident that they can quit in the next
month decreased significantly from 2001 to 2006. Only 26.3% of smokers are seriously thinking
of quitting smoking in the next 30 days. In 2006, 52.7% of current smokers and recent quitters
reported a serious quit attempt in the last 12 months. This percentage has not changed
significantly since 2001. Because most smokers make five to seven attempts before successfully
quitting, it is important for smokers to continue to try to quit.
There has been no significant change since 2003 in the percentage of current smokers who used
the Quit Line or group counseling during their quit attempts in the past 12 months (Exhibit 8).
Exhibit 8: Percentage of Current Smokers Who Seriously Tried to Quit in the Last 12 months Using the
Quit Line and Group Counseling
Approved pharmacotherapy doubles the success rate of a quit attempt. Encouragingly, the percentage of current smokers who have never used pharmacotherapy (nicotine replacement therapy (NRT), Zyban or Chantix) has decreased significantly over time (Exhibit 9), though it still remains high. EXHIBIT 9: Current Smokers Who Have Never Used NRT, Zyban or Chantix 2002-2006 (VT ATS)
Never used NRT, Zyban, or Wellbutrina
Notes: 2002 ATS did not include Zyban or Wellbutrin, and 2006 ATS included Chantix.
This question was not asked in the 2001 ATS.
aSignificant linear trend.
Health Care Providers: Need to Refer More Smokers to Cessation Services
Health care providers are the most credible source of messages about health, and have the
opportunity to address smoking. In 2006, nearly 70% of Vermont smokers reported that they
visited a health care provider at least once in the past 12 months. Tobacco use screening with
brief physician intervention is one of the three highest ranking preventive services in both
cost effectiveness and reducing adverse health events. Although 80% of smokers reported that
their health care provider asked if they smoked, only 30.1% were recommended a specific
medicine or program. This percentage has increased over time but it is still low (Exhibit 10).
EXHIBIT 10: Current Smokers Who Were Recommended a Specific Medicine or Program by their Health Care Provider in the Past 12 Months. 2001 – 2006 (VT ATS)
More work is needed to educate providers about the efficacy of available cessation services and to encourage them to refer patients to these services. The board endorsed a proposal from the Cessation Committee for health care provider training, and funding was allocated in FY2007 to initiate a pilot program. This program is explained in more detail in Section III of this report under "Statewide Training of Health Care Providers".
EXPOSURE TO SECONDHAND SMOKE DECLINES
Among smokers, the trend in total home smoking ban among Vermonters as a whole, with or
without children, has increased over time, although the trend in both groups has leveled off
(Exhibit 11).
EXHIBIT 11: Percentage of Vermont Smokers Reporting Smoke-Free Policies in the Home,
2001 – 2006 (VT ATS)
Among all Vermonters with children, the proportion with smoke-free vehicle policies rose from
80% in 2001 to 89.3% in 2006 (Exhibit 12). Since 2004, the Department of Health has
implemented the fall common theme campaign, Smoke-Free Zone, to encourage adults to create
smoke-free environments near children, inside and out.
EXHIBIT 12: Percentage of Vermonters with Smoke-Free Policies for Cars, 2001 – 2006 (VT ATS)
III. EVALUATION OF PROGRAM COMPONENTS
TOBACCO-FREE COMMUNITY COALITIONS
There are currently 19 tobacco-free community coalitions funded by the Department of Health
(Exhibit 14). Grants for coalitions are awarded on a competitive basis. A description of the
process for developing the Request for Proposal and reviewing proposals is included in Section
IV of this report.
Over 60% of the current coalitions have been funded since FY2001 and are well established in
their communities; the other grantees have received awards for several years. Although most
towns in Vermont are served by a coalition, there are gaps in service including sections of
Chittenden and Bennington counties and Essex, Orange, Orleans, Windsor and Windham
counties.
Goals
The goals of the coalitions mirror those of the statewide Tobacco Control Program:
To prevent young people from starting to smoke
To link people with resources and services to help them quit smoking
To reduce the exposure of all Vermonters to secondhand smoke
Community coalitions tailor strategies and activities to address each goal based on local needs
and resources. In January 2003, the Department of Health (VDH) implemented a
recommendation of the independent evaluation contractor, Research Triangle Institute (RTI), to
require all community coalitions to participate in common theme campaigns. Coalitions design
and conduct activities at the local level that complement the theme of the statewide media
campaign airing during a specified period. Common theme campaigns strengthen the core
message (see Media and Public Education in this section) by delivering it through multiple
channels statewide during a designated period.
Community Coalition Activities
In FY2006, the community coalitions reporting forms were revised to collect data that would
provide a more accurate picture of the mix of coalition activities across the statewide program
goals. Because coalitions were able to select more than one statewide program goal prior to
FY2006, they may have attributed some activities to more than one program goal. In FY2007,
community coalitions conducted 740 activities addressing all three tobacco control program
goals. Of these activities, 42.3% addressed youth prevention, 31.1% addressed smoking
cessation and 18.9% addressed secondhand smoke (Exhibit 13). Despite VDH requirement that
community coalitions focus greater efforts toward cessation and secondhand smoke activities,
the imbalance of activities in favor of youth prevention has been persistent over time.
Collaboration
Although the coalition activities are disproportionately geared toward youth prevention, the
coalition data show considerable collaboration with a wide variety of organizations.
Educational organizations, such as schools and colleges have been the most frequent type of
collaborator. Nearly every coalition collaborated with an educational organization to conduct 172
of the 740 activities completed in FY2007. Healthcare organizations and providers have also
been frequent collaborators, working with 139 of the 740 activities in FY2007.
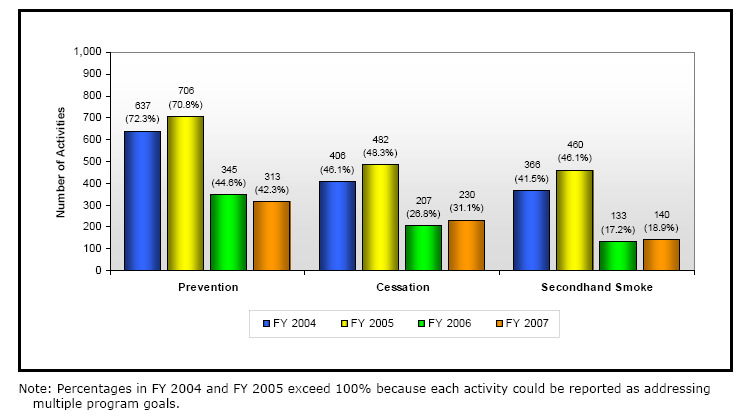
A vast majority of coalitions also collaborated with state agencies such as VDH, the Department of Liquor Control, and law enforcement. A large number of collaborators have not yet been classified. RTI recommends a review by VDH to provide a more accurate understanding of the types of organizations that community coalition work with to conduct tobacco control activities. During FY2007, the 19 tobacco coalition coordinators completed the Community Capacity Assessment Survey to help provide a developmental snapshot of each coalition. After completing the survey, each of the coalitions worked with one of two VDH consultants to assess survey results. The contractors offered technical assistance to strengthen and increase each coalition's active membership and to assist them in operating at the fullest potential within their community. Coalition coordinators utilized feedback from the contractors to develop objectives and activities in their FY2008 work plan, specifically to enhance coalition membership and address populations with disparately high smoking rates. EXHIBIT 13: Community Coalition Activities by Program Goal Addressed, FY2004 – FY2007. Prior to FY06 when data collection system was revised, some activities may have been over reported.
EXHIBIT 14: Community Coalition Grants by County, FY2008
Coalition/Fiscal Agent
Addison County
Addison County Tobacco Round Table (Community Health Services of Addison
Bennington County
Bennington Stamp Out Tobacco Coalition (Center for Restorative Justice)
Caledonia County
Community Coordinating Council (Northeastern VT Regional Hospital)
Chittenden County
Chittenden East Community Partnership (Chittenden East Supervisory Union)
CY: Connecting Youth (Chittenden South Supervisory Union)
Milton Community Youth Coalition
Franklin County and Grand Isle County
Franklin Grand Isle Tobacco Prevention (Northwestern Medical Center)
Lamoille County
Lamoille Valley Tobacco Task Force (Copley Professional Services Group, Inc)
Orange County and Washington County
Gifford Community Tobacco Free Coalition (Gifford Medical Center)
Orleans County and Essex County
Health & Traffic Safety for ONE (North Country Hospital )
Rutland County
Rutland Area Prevention Coalition (Rutland Community Programs)
Washington County
Cabot Community Association
Central Vermont New Directions (Washington Central Friends of Education)
New Directions for Barre
Windham County
Communities Against Tobacco Brattleboro (Southern VT Health Services)
The Collaborative (Mountain Communities /dba Flood Brook Community
Windsor County
Mt. Ascutney Prevention Partnership (Windsor Hospital dba Mt. Ascutney
Hospital and Health Care) STOP: Springfield Tobacco Options & Prevention (Health Care and
Rehabilitative Services)
TOTAL
$1,003,328
YOUTH EMPOWERMENT PROGRAMS
The Department of Health (VDH) administers two statewide anti-tobacco programs that promote
positive youth development through peer leadership and youth empowerment in addressing the
problems of tobacco use.
Vermont Kids Against Tobacco (VKAT): Middle School Youth
Since 1995, VKAT groups of youth in grades 6 through 8 have been devoted to keeping
themselves and their peers tobacco-free. VKAT is funded from the Centers for Disease Control
and Prevention (CDC) annual grant to VDH. VKAT groups create activities to inform their
peers and their communities about the hazards of smoking and to support tobacco-free choices.
For example, VKAT groups conduct media literacy training, talk to legislators about the
importance of tobacco prevention at the VKAT annual statehouse rally and implement activities
to counter tobacco industry marketing to youth.
There were 39 sites funded in the FY2001, 48 in each of the next two years, 54 sites in FY2004,
and 57 in FY2005 and FY2006. Due to a decrease in CDC funding, 51 sites were awarded grants
in FY2007 and FY2008 (Appendix 4).
Our Voices Xposed (OVX): High School Youth
In August 2000, Vermont was awarded a three-year grant totaling $1.5 million from the
American Legacy Foundation (ALF) to support a statewide teen movement against tobacco.
Vermont teens selected the name for the movement, Our Voices Xposed (OVX). They have
provided leadership and momentum from the outset. OVX is open to high school youth who
want to get involved to reduce tobacco use among their peers, 13- to 18-year-old Vermonters.
The goals of OVX are to:
Educate and inform
Empower and show teens how to express their views
Take action against the exploitation of the tobacco industry
Encourage positive behavior in all aspects of life
Help reduce tobacco use among our peers
The ALF grant funded at least 25 OVX sites from 2000-2003. It also funded a professional
media campaign designed by VDH and its media contractor in collaboration with OVX. This
non-renewable grant ended in August 2003 and VDH used unexpended grant money to continue
funding some OVX activities but no media campaigns. Since 2006, the Department of Health
has received some support through the CDC grant award and currently funds 10 OVX sites
(Appendix 4).
The Department of Education offers small grants to schools for the Vermont Teen Leadership Safety Program (VTLSP) to address tobacco use among teens. The Departments of Health and Education coordinate efforts through the annual youth prevention common theme campaign.
SCHOOL-BASED TOBACCO USE PREVENTION PROGRAMS
The Department of Education (DOE) administers the school-based tobacco use prevention
program. Schools play a major role in the statewide effort to reduce the initiation and use of
tobacco by youth and help to create community and school environments where "No Tobacco" is
the norm.
Goals
The four interventions included in the school-based tobacco use prevention program are:
1. School Tobacco-Free Policy A comprehensive policy on tobacco use that is well understood and consistently enforced is the foundation for an effective school-based tobacco use prevention program. A model policy developed with students, parents, school staff, law enforcement and health professionals will:
Explain the health reasons for a tobacco-free policy.
Specify how the policy will be communicated.
Prohibit students, parents, staff and visitors from using tobacco on school grounds, in school vehicles and at school events.
Prohibit tobacco sponsorships of/or advertising at school events.
Provide instruction on refusal skills needed to prevent tobacco use.
Provide students and staff who violate alcohol, tobacco and other drug (ATOD) policies with options that may include cessation programs.
2. Curricula The school-based prevention grants support schools in implementing research-based tobacco prevention curricula to:
Encourage schools to include research-based tobacco prevention curricula as part of a comprehensive health education program.
Support and arrange for training of educators in research-based tobacco prevention curricula.
Encourage and promote delivery of curricula with fidelity shown most effective in reducing tobacco use.
3. Parent and Community Education Schools continue to work in partnership with community-based coalitions, service providers, family physicians and youth empowerment groups in expanding prevention efforts.
Schools and Vermont Teen Leadership Safety Program (VTLSP) groups across the state have joined in common theme prevention campaigns.
Schools provide information about local policy, prevention needs and prevention activities.
4. Cessation As schools work to prevent young people from smoking and enforce a tobacco-free policy for staff, it is critical to have resources to help those who want to quit smoking
Schools offer youth smoking cessation services and refer adult smokers to community quit smoking resources. See Section III under "Smoking Cessation Services" for more information about both programs.
In FY2007, Student Assistant Professionals (SAPs) programs within schools referred 232 students to smoking cessation programs.
As of September 2007, teens can call the Vermont Quit Line, without parental consent, for free counseling to quit smoking.
Grants
DOE invites all of the supervisory unions (SUs) and school districts (SDs) in the state to apply
for non-competitive grants. The size of the grants is determined by a formula based on student
enrollment, with a minimum grant of $5,000. Independent schools may also apply. In FY2007,
92% of supervisory unions, school districts and independent schools received tobacco prevention
school grants (Exhibit 15).
EXHIBIT 15: School-based Tobacco Grants by County*: Estimated Funding FY2008
* Some grantees serve town(s) in an additional county.
Supervisory Union/School District/Independent School
Grant FY2008
Addison County
Bennington County
Bennington-Rutland*
Burr & Burton Academy
Caledonia County
Blue Mountain* Caledonia & Orange Counties
Caledonia Central
Lyndon Institute
St. Johnsbury/St. Johnsbury Academy
Chittenden County
Chittenden Central
Chittenden South
has not applied
South Burlington
South Burlington – Rice Memorial High School
Essex County
Essex-Caledonia* (Essex & Caledonia)
Franklin County
Franklin Central
Lamoille County
Supervisory Union/School District/Independent School
Grant FY2008
Orange County
has not applied
Rivendell * includes Grafton NH
Orleans County
Orleans-Essex North *(Brighton only in Essex County)
Orleans SW * (Orleans, Caledonia, Lamoille and Washington)
Rutland County
Rutland NE * (Addison and Rutland)
Rutland-Windsor * (Rutland and Windsor)
has not applied
Washington County
Washington Central
Washington South
Windham County
Windham SW *(Bennington and Windham)
Windsor County
has not applied
Thetford Academy
Windsor Central * (Windsor and Rutland)
Windsor NW * (Addison, Windsor, and Rutland)
Windsor SW * (Bennington, Windham, and Windsor)
Total Grants to Supervisory Unions:
$772,284
Tobacco Coordinator Training and GYLC
Professional Services and Other Expenses
$995,668
Activities
Coordination: The key to the demonstrated success of this program is the tobacco coordinator
who works part-time (typically six to eight hours per week) in the SU or SD. Among the 59 grant
sites, the coordinator turnover rate between the FY2006 and FY2008 grant years is 22% to date.
The department provided orientation and on-site technical assistance for new coordinators. Many coordinators are also Student Assistance Professionals (SAP) and work directly with students, assisting with prevention curriculum and providing referrals to cessation services. Tobacco-free Policy: According to the Centers for Disease Control and Prevention (CDC), interventions to prevent tobacco use initiation and encourage cessation among young people need to reshape the environment so that it supports tobacco-free norms. At the end of FY2007, 296 of 317 (93.7%) public and independent schools in funded supervisory unions and school districts had a tobacco-free policy in place. Curricula: Vermont's Tobacco Control Program supports five evidence-based curricula including the Michigan Model for Comprehensive School Health, Project Towards No Tobacco Use, Teenage Health Teaching Module, Life Skills Training and Know Your Body. The percentage of students enrolled in research-based tobacco prevention curricula has remained steady since FY2004 and increased from FY2006 to F2007 (Exhibit 16). Exhibit 16: Implementation of Research-based Tobacco Use Prevention Curricula, FY2000-FY2007
Parent and Community Education: In FY2007, 18,346 students and 803 staff in 201 schools engaged in a common theme campaign, in coordination with the Department of Health and local tobacco coalitions. Reports from schools indicate this is one of the greatest areas of success as it engaged students statewide. Based on the board's recommendation, the Legislature appropriated funds to implement a tobacco prevention track at Governor's Youth Leadership Conference the last two years. On November 19, 2007, 427 students from across the state attended this daylong event, and 101 of them participated in the tobacco prevention track. Speakers linked upcoming prevention themes and activities for youth with brainstorming and educational sessions that relate directly to this year's common theme campaign, Correcting Misperceptions.
SMOKING CESSATION SERVICES
Vermont's comprehensive tobacco control program promotes smoking cessation through
multiple channels: community coalitions, mass media, direct mail, health care provider referrals,
inpatient visits to patients who smoke, and other educational efforts. Free smoking cessation
counseling services are available for all tobacco users, although cigarette smokers comprise the
majority of tobacco users in Vermont. The program offers help to adult smokers in four ways:
Vermont Quit Line
Hospital-based cessation counseling
Vermont QuitNet web-based support
Free or discounted nicotine replacement therapies (NRT)
Vermont Quit Line (1-800-QUIT-NOW): The American Cancer Society's National Cancer
Information Center has operated the Vermont Quit Line under a contract with the Department of
Health (VDH) since February 2001. It also operates quit lines for several other states, although
information is tailored for each state program. Calls are answered 24 hours per day, every day of
the year. Counselors are available Monday through Thursday from 7:00 a.m. to midnight and
Friday through Sunday, 7:00 a.m. – 9:00 p.m.
Some callers are only interested in receiving specific information in response to their questions.
Some smokers prefer to quit on their own and are sent a packet of self-help materials. For
smokers interested in quitting and prefer the convenience and anonymity of telephone
counseling, the Quit Line provides a research-based, five-session counseling program. For
smokers interested in face-to-face programs, the Quit Line refers them to the Vermont hospital
nearest to them.
Hospital-based Program: VDH contracts with Fletcher Allen Health Care to oversee the
smoking cessation program, Ready, Set…STOP, at Vermont's 13 hospitals (Exhibit 17).
Counselors offer group or one-to-one counseling sessions. Through a collaboration of the
Vermont Association of Hospitals and Health Systems and the American Cancer Society, Ready,
Set…STOP adapted the six-session Freshstart Program for use in the statewide hospital-based
program.
Quit Line and Ready, Set…STOP provide up to eight weeks of NRT (patches, gum and
lozenges) to adult smokers who enroll in counseling.
EXHIBIT 17: Ready, Set…STOP Grants to Hospitals, FY 2008
Hospital
FY2008 Grant
Brattleboro Memorial Hospital
Central Vermont Medical Center
Fletcher Allen Health Care
Gifford Hospital
Mt. Ascutney Hospital
North Country Hospital
Northeastern Vermont Regional Medical Center
Hospital (continued)
FY2008 Grant
Northwestern Vermont Medical Center
Rutland Regional Medical Center
Southwestern Vermont Healthcare
Springfield Hospital
Total Grants
$602,715
QuitNet (www.vt.quitnet.com): This is a web-based smoking cessation service, owned by
Healthways, Inc. and operated in association with Boston University School of Public Health.
VDH has contracted with Healthways, Inc. since September 2005. QuitNet develops an
individual smoking cessation plan from information the smoker provides on a secure website.
Vermonters who register with QuitNet have a free lifetime membership. In addition, information
about Vermont's other services appear on the screen whenever any smoker from Vermont
registers with QuitNet.
Nicotine Replacement Therapy (NRT): The average smoker will attempt to quit five to seven
times before succeeding. Most smokers try to quit on their own despite the fact that only 3% to
5% of people who try to quit unaided will succeed. Over 120 research studies show that
medication - such as NRT and buproprion - double the success rate of quit attempts. Combining
medications with counseling and follow-up further increases the success rate. For several years,
the board has recommended that free NRT (a non-prescription medication) should be available to
every smoker who enrolls in counseling.
The distribution of NRT has evolved over time. In 2001, VDH began the "Quit Bucks" program
- coupons for free or discounted NRT redeemable at local pharmacies - by providing the
subsidies only to the uninsured and Vermont Health Access Program (VHAP) enrollees. Over
time, additional groups (Medicare, Ladies First Breast & Cervical Program clients) became
eligible. In 2002, VDH developed a pilot program with private insurers who agreed to reimburse
a portion of NRT cost for Quit Bucks coupons for their subscribers. Utilization of that partial
benefit was low and there was evidence that subscribers were largely unaware of it. In 2004, the
Attorney General provided additional funding and "Quit Bills" were created. These coupons
covered the remaining NRT costs for smokers with a partial benefit, and provided some coverage
for smokers not previously included.
New guidelines for NRT distribution have been issued periodically to hospital counselors, who
sorted through complicated eligibility requirements to provide fully subsidized NRT to most of
the smokers enrolled in counseling. This was a cumbersome process and may have been a
disincentive for smokers. VDH and Vermont Association of Hospitals and Health Systems
(VAHHS) worked to identify simpler and less expensive mechanisms for providing NRT to
smokers enrolled in counseling.
As of February 1, 2007, the Quit Line and Ready, Set…STOP offer direct shipment of free NRT
to most all smokers who agree to counseling, regardless of insurance coverage. The only
exception is Medicaid and Vermont Health Access Program (VHAP). These beneficiaries are
required to get a prescription from their physician and pay a co-pay of $2.00.
Utilization of Services
New Clients: The number of new clients served by the Quit Line, Ready, Set…STOP and Quit
Net in the past three fiscal years is provided in Exhibit 18. These figures do not fully represent
the volume of services provided. In any given year, the programs serve new clients, as well as
clients whose counseling bridges more than one year and those who relapsed to smoking and
have returned for additional support.
EXHIBIT 18: New Clients Served by Quit Line, Ready, Set.STOP and QuitNet, FY2005 - FY2007
FY2005 FY2006 FY2007
Quit Line
Self Help Materials Mailed
Information Only
Quit Line Subtotal
Ready, Set…STOP
NRT only (Quit Line clients)
Not Counseled nor NRT
Ready, Set.STOP Subtotal
Registered Members
Total New Clients*
*To avoid double counting, Quit Line clients who received NRT from Ready, Set.STOP are not included in totals. **10 months only There has been a steady upward trend in the number of Vermont smokers enrolled in Ready, Set…STOP from FY2004 – FY2007. From FY2006 to FY2007, there was an increase of 30% in the number of smokers counseled. Until FY2005, the number of smokers counseled through Ready, Set…Stop was roughly comparable to number of smokers receiving phone counseling through the Quit Line. However, from FY2005 on, the decline in the number of clients counseled by the Quit Line has corresponded to an increase in Ready, Set…Stop clients. In addition, hospital counselors visited 3,866 hospital patients that smoke to encourage a quit attempt. These visits are not included in the data contained in Exhibit 18. Despite the decline in the number of smokers counseled by the Quit Line, the annual call volume increased by almost 4% in FY2007. The Quit Line call volume was relatively stable in FY2005 and FY2006, but the increase in calls in FY2007 may be an early indicator that call volume could be on the rise again. According to RTI, the independent program evaluator, the trends in Quit Line and Ready, Set…STOP client totals suggest that a relatively consistent and perhaps even increasing percentage of Vermont smokers are receiving counseling services.
Reach of Cessation Services
The reach of a program is defined as the percentage of the target population served by that
program in a defined period of time. About 4% of Vermont smokers used one of the state's quit
smoking services (Exhibit 19). The reach of both programs is greatly affected by promotion of
the service through mass media campaigns and direct mail (See "Media and Public Education" in
this section).
Exhibit 19: Reach of Cessation Services, FY2007
Cessation Service
(Number of Smokers Enrolled, FY2007)
Percentage of Estimated Smokers3
Quit Line (1,421)
Ready, Set…STOP (1,936)
12.8% of QuitNet users are 18-24 year olds, similar to the Quit Line (11.6%).
11.4% of Quit Line clients have less than a high school degree compared to 15.4% of Ready, Set…STOP clients.
54.3% of Ready, Set…STOP clients are 45 years or older compared to 44.9% of Quit Line clients.
Over half of the Ready, Set…STOP and Quit Line clients are female.
Over 64% of Quit Net users are female.
41.3% of Ready, Set…STOP clients have some college education or more compared to 44.1% of Quit Line clients.
68.2% of QuitNet users have some college education or more.
Efficacy of Services
Follow-up Calls: The American Cancer Society attempts to reach every smoker who received
Quit Line services with follow-up calls. VDH contracts with Macro International to conduct the
follow-up calls with Ready, Set…STOP clients, using a similar model of attempting to reach
every caller. Follow-up calls are designed to assess smoking status and satisfaction with services.
Calls for both programs are made approximately three, six, and 12 months after completion of
the services (Exhibit 20).
EXHIBIT 20: Rates of Completion of Follow-up Contacts with Counseling Clients
Follow-up Contacts
Quit Line FY2005
Ready, Set…Stop FY2007
Definition of Quit: The standard method for calculating the rate of quitting is to assume that all
clients who could not be reached for a follow-up telephone interview have relapsed to smoking.
Thus, achieving high quit rates is greatly dependent on successfully reaching clients to complete
the follow-up interviews.
The second method of calculating the rate of quitting is to exclude all clients who were not
reached in the follow-up, and report the percentage of clients who quit among those reached in
follow-up. Exhibit 21 shows Quit Line and Ready, Set.STOP quit rates using both methods.
3 Behavioral Risk Factor Surveillance Survey, 2006
EXHIBIT 21: Quit Rates for Current Smokers Counseled by the Vermont Quit Line and Ready, Set.STOP, 7-day point prevalence (smoke free 7 days prior to telephone contact)
Ready, Set.STOP,
Quit Line, 2006
3-Month Follow-up
Eligible for follow-up
Completed follow-up
6-Month Follow-up
Eligible for follow-up
Completed follow-up
12-Month Follow-up
Eligible for follow-up
Completed follow-up
Exhibit 21 shows that the quit rates are higher for Ready, Set.STOP clients than Quit Line
clients. Given the differences in the types of smokers who join Ready, Set.STOP and Quit Line,
the intensity of the two treatments and the follow-up rates for the two programs, the board's
Evaluation Committee does not use the quit rates of the two programs to compare
their effectiveness. Smoking cessation researchers who serve on the board's Cessation
Committee concluded that the quit rates for both programs are excellent.
Client Satisfaction with Smoking Cessation Services
The Quit Line and the Ready, Set.STOP programs have consistently received very high
satisfaction ratings from their clients. This data is gathered during the first follow-up call
completed with the client. Since about 50% of clients counseled are not reached during
follow-up, the satisfaction levels of about half of the clients counseled are not known. However,
among those reached during follow-up, the reported satisfaction levels for those counseled by the
Quit Line average over 8.5 (on a scale of 0 to 10) for a 10-item measurement protocol.
Satisfaction levels with the Ready, Set.STOP program are equally high. Among clients reached
for follow-up between July 2006 and June 2007, 85% were satisfied or very satisfied with the
support received from the program; 83% found the counselor helpful or very helpful. Among
those that took a group class, 81% found those classes helpful or very helpful.
Coordination of Cessation Services
The hospital-based program originally offered group counseling only. Over time, it added
face-to-face counseling and telephone counseling and a combination. Each hospital is required to
offer at least six group cessation programs per year, half of those in community or worksite
settings. In FY2007, the hospitals offered a total of 221 group programs, an increase of 8% from
the previous year. In FY2007, 78% of groups were completed, compared to 74% in FY2006. In
addition, more smokers completed a group program in FY2007 (972 smokers) than FY2006 (712
smokers). In spite of the increase in group counseling, approximately 35% of new clients were
counseled exclusively by telephone in FY2007.
VDH and the board have been concerned about this shift to phone counseling offered by the
hospitals and duplication of Quit Line services. In December 2007, VDH convened a Scientific
Advisory Panel to 1) examine Vermont's cessation program by reviewing the data and outcomes;
2) compare the coordination of Vermont's cessation services to other states and; 3) develop
recommendations for VDH to address coordination and efficiency among cessation providers.
VDH and the board will review the panel's recommendations in the winter of 2008 and VDH
will make a final set of determinations about coordinating these programs by the end of FY2008.
Youth Cessation Programs
Most of the smoking cessation services in Vermont are targeted to adult smokers. In 2007,
legislation was passed to allow smokers under the age of 18 to call the Quit Line for counseling
without parental consent. As of September 1, 2007, teens may register for the Quit Line's
smoking cessation counseling designed for smokers under the age of 18.
Two teen smoking cessation programs are currently available in Vermont. The demand for teen
smoking cessation programs among teachers and community members is high; yet it is often
challenging to recruit students and find time during the school day to schedule these programs.
Not On Tobacco (N-O-T): N-O-T is a research-based program designed specifically for teenage
smokers by the American Lung Association. Evaluation research published in a peer-reviewed
journal in 2005 demonstrated the efficacy of the program4. N-O-T includes 10 weekly group
sessions and four optional booster sessions. It was designed to be gender-specific with separate
groups conducted for male and female teens by facilitators of the same gender. This design has
been adapted for small group sessions in a rural state like Vermont. N-O-T is a voluntary
program.
Since 2001, VDH has contracted with the American Lung Association of Vermont (ALA-VT) to
provide N-O-T at high schools and other sites that reach nontraditional students and high-risk
youth. ALA-VT signed agreements with 41 sites to offer N-O-T in FY2007. 50 people,
primarily school staff, were trained to facilitate the program. Of the 41 sites, 25 completed at
least one ten-week group for a total of 38 groups. Of the 231 teen smokers who started N-O-T,
166 finished the program and completed the post-survey.
Tobacco Awareness Program & Tobacco Education Group: The Department of Education
(DOE) allows tobacco prevention grant recipients to expend grant funds to implement the
Tobacco Awareness Program (TAP) and the Tobacco Education Group (TEG) interventions in
their schools. TEG is designed as an alternative to suspension for students caught using tobacco
on school property. It includes eight sessions designed to motivate students to quit using tobacco
or to join the TAP program. TAP is a voluntary tobacco group focused on stopping smoking or
using other tobacco products as well as on behavior modification.
To date, more schools use N-O-T as the program of choice for youth smoking cessation. The
DOE program coordinator has encouraged grantees to consider N-O-T because of the support
system provided by the ALA-VT (mini-grants, training, technical assistance, incentives and data
collection).
4 Horn H, Dubi Gm Kalsekar I, Mody R. (2005). The impact of Not on Tobacco on teen
smoking cessation: End-of-program evaluation results, 1998-2003. Journal of Adolescent
Research 20 (6): 640-661.
STATEWIDE TRAINING OF HEALTH CARE PROVIDERS
Health Care Provider Training
There was an initiative to train physicians and other health care providers during the initial three
years of the Vermont Tobacco Control Program. That program was terminated by mutual
agreement between the training organization, Area Health Education Centers (AHEC), and the
Vermont Department of Health (VDH) in June 2003. The program was a fairly intensive
intervention that required a time commitment on the part of physicians that most were unwilling
or unable to make. The board was concerned that too few providers could be reached with this
intervention with the available funds. It recommended that the Legislature shift the funds to
provide subsidies for nicotine replacement therapy (NRT) for more smokers who enrolled in
counseling.
Health care providers are the most credible source of health care advice. First, current smokers
identify health care providers as important sources of information about cessation assistance.
Second, physicians and other health care providers have frequent opportunities to intervene with
current smokers. Nearly 70% of Vermont smokers reported in 2006 saw a health care provider
during the past 12 months. Third, according to the National Commission on Prevention
Priorities, tobacco use screening with brief physician intervention by physicians are both highly
efficacious and cost saving in comparison to other prevention services.
Although most smokers reported visiting a health care provider in 2006, only 30% of current
smokers reported their health care provider recommended a specific medicine or program for
quitting smoking. More work is needed to educate health care providers about smoking cessation
counseling and medications, and to increase their referrals to Vermont's cessation services.
At the board's recommendation, $75,000 was appropriated in FY2007 and again in FY2008 to pilot a more efficient method of health care provider training. VDH contracts with John Snow International (JSI) to replicate a very successful model from Massachusetts. In Vermont, JSI is working with clinics to institute a systems change to identify and refer smokers to the Quit Line or the hospital program. For those smokers who may not want to quit using counseling, JSI provides nicotine replacement therapies (NRT) to these practices, in order to increase the smoker's chance for success by using medication. JSI has provided training to:
Northern Tier Center for Health, a Federally Qualified Health Center (FQHC) with clinics in Alburgh, Enosburg, Richford and Swanton.
Six Vermont Clinics for the Uninsured: People's Health and Wellness (Barre), Park Street Healthshare (Rutland), Open Door (Middlebury), Good Neighbor (White River Junction), Precision Valley Healthcare (Springfield) and Windsor Community Health Clinic.
Other clinics have expressed interest, including the Community Health Center of Burlington. JSI provides online orientations for providers through the Vermont Program for Quality in Health Care, Inc (VPQ) to encourage participation in the program and NRT distribution. Fax Referrals: Health care providers can refer smoking patients to the Quit Line or hospital counseling via a confidential fax referral system. Health care providers secure the patient's permission to fax a referral to the Quit Line and Ready, Set…STOP and a counselor will call the smoker to encourage enrollment into counseling.
In FY2007, 30.2% of patients referred by health care providers to the Quit Line completed an intake and 57% of patients referred by health care providers to local hospitals enrolled in Ready, Set.STOP (Exhibit 22).
Exhibit 22: Total number of fax referrals from health care providers to the Quit Line
and Ready, Set.STOP program, FY2006 and FY2007.
Cessation Service
# of faxes
# of intakes
# of faxes
# of intakes
Dental Provider Training
The Vermont State Dental Society has conducted training programs for dental office staff since
April 2001 under a contract with the Department of Health. The goals of these office-based
trainings are to ensure dentists and their office personnel:
Ask at every visit whether or not the patient smokes
Advise patients who smoke to quit
Assist smokers by referring them to cessation services
The dental society has trained 192 (83%) of the 236 dental offices in Vermont and returned to 80 offices for refresher trainings (Exhibit 23) since the program began. Since the dental society has trained most of the practices in the state, it now spends more time updating each practice with current information to ensure that referral practices remain in place. EXHIBIT 23: Number of Dental Office Trainings Conducted and Staff Trained by Vermont State Dental Society, October 2001 – June 2007
Training
In FY2007, 10% of fax referrals to the Quit Line came from dental providers. Smokers referred to counseling by a dental provider are more likely to enroll in the program than smokers referred by other sources (78% of referrals by dental providers enroll in counseling compared to 30% for all referral sources).
MEDIA AND PUBLIC EDUCATION
Tobacco companies spend billions annually to make tobacco use appear to be an attractive and
established part of American culture. The three most heavily advertised cigarette brands account
for more than 80% of cigarettes smoked by adolescents5. Media and public education are key
components of Vermont's Tobacco Control Program. These interventions are powerful tools to
counter the marketing effects of the tobacco industry and to educate the public. The Vermont
Department of Health (VDH), in collaboration with the media contractor, Kelliher Samets Volk
(KSV), develops and implements an annual media and public education plan.
Health communications are more effective when the message is delivered from multiple sources.
As a result, VDH conducts three statewide common theme media campaigns per year in concert
with community and school public education activities. Each campaign focuses on a particular
theme during a designated time period and mirrors one of the three statewide tobacco control
goals:
Goal 1: Prevent youth from starting to smoke
The long-range objective of all prevention campaigns is to cut youth smoking rates in half
between 1999 and 2010. The 1999 smoking rate for grades 8 through 12 was 31%. The 2007
smoking rate was 16% (a 48% drop). The 2010 goal is 15%.
Goal 2: Help smokers to quit
The long-range objective of smoking cessation campaigns is to reduce the adult smoking
prevalence rate by half between 1999 and 2010. The smoking rate in 1999 among adults 18 and
over was 22%. In 2006, the smoking rate among adults 18 and over was 18%. The goal for 2010
is 11%.
Goal 3: Reduce exposure of all Vermonters to secondhand smoke
The goal is to reduce secondhand smoke exposure for all Vermonters, with a focus on reducing
exposure of youth. Adult Tobacco Survey (ATS) data indicate that exposure to secondhand
smoke in the home has steadily declined in Vermont. However, this favorable trend in the
percentage of smokers prohibiting smoking in their homes has leveled off among households
with and without children.
The FY2008 Common Theme Campaigns are:
Correcting Misperceptions: See Youth Prevention (Ages 10 to 13)
Every Try Counts: See Smoking Cessation (Ages 25 to 34)
Smoke-Free Zones: See Reduce Exposure to Secondhand Smoke
FY2008 Media & Public Education Plan
Youth Prevention (Ages 10 to 13)
The 8 out of 10 (Correcting Misperceptions) campaign was developed to help correct a
commonly-held and powerful belief among tweens (ages 10 to 13) that most high school students
smoke. Initiated in 2001, Correcting Misperceptions is now one of three annual common theme
campaigns.
5 Substance Abuse and Mental Health Services Administration (SAMHSA), The National Survey on Drug Use and Health Report. SAMHSA Office of Applied Studies, Washington DC; 2007.
This year's campaign will take place in March and April. The media, including television spots, is designed to inform youth about the facts of youth smoking and guide them to the 8outof10.com website. This site will have links to other sites, including Vermont Kids Against Tobacco (www.govkat.org) and Our Voices Exposed (www.ovx.org). To ensure statewide coordination of this common theme campaign, community partners will be given campaign briefs, giveaway items, campaign images, downloadable resources, a press release template and talking points, a classroom guide, and idea lists.
Youth Prevention (Ages 10 to 13)
Objectives: To reinforce anti-tobacco attitudes and decrease the proportion of middle school
students intending to initiate smoking
Primary target: Ages 10 to13
Secondary target: Ages 14 to17
Marketing vehicles: TV ads, print, website
Campaign Partners: community coalitions, Department of Education, Vermont Kids Against
Tobacco (VKAT) and Our Voices Exposed (OVX) youth empowerment groups
Evaluation tools: Youth Health Survey (YHS) and Youth Risk Behavior Survey (YRBS)
Media Timing: March and April 2008 (media will begin in mid-February).
Youth Prevention (Ages 14 to 17) Last year, the common theme campaign, Butts of Hollywood, focused on how tobacco use in the movies influences opinions and smoking initiation among youth. Although this year's common theme campaign, Correcting Misperceptions, will target tweens, it is important to continue to counter among older adolescents the estimated $36.7 million that tobacco companies spend each year in Vermont on tobacco marketing. OVX groups, community coalitions, and school-based tobacco use prevention coordinators will sponsor community-level activities when this campaign airs, some coinciding with the Academy Awards. The campaign will use existing Butts of Hollywood television spots and will guide youth to the OVX website's (www.ovx.org) interactive game. Existing promotional materials will be distributed to the OVX groups, coalitions and schools. VDH provides partners with a media literacy guide, Media Revealed: Understanding our Media Diet. The guide enables partners to deliver presentations and educate community members about today's media landscape and ways to protect youth from media influences that promote harmful behaviors.
Youth Prevention (Ages 14 to 17)
Objectives: To increase awareness about tobacco advertising targeted to youth in order to
empower teens to be smart consumers of media.
Primary target: Ages 14 to17
Secondary target: Ages 10 to 13
Marketing vehicles: Existing TV spots, giveaway items, website
Community Partners: OVX, community coalitions (not required) and Department of Education
(not required)
Evaluation tools: Youth Health Survey, Youth Risk Behavior Survey, website visits, material
distribution, measured media, total number of community events
Media Timing: January and February 2008
Smoking Cessation (All Adult Smokers) The overall adult smoking rate dropped to 18% in 2006, the first significant decrease since 2000. However, quit attempts among smokers and recent quitters have fallen slightly in the last year, with just over half making a serious quit attempt. In addition, fewer adults with a high school education or less are trying to quit, and their rate of smoking is higher than the overall rate. According the 2006 ATS, a majority of Vermont smokers prefer to quit smoking on their own. Media and educational materials will be created or updated to provide smokers who do not intend to use Vermont's smoking cessation services tools that will help them in their quit attempts. Previously-developed materials and campaigns also will be implemented in FY2008:
Direct Mail: a mailer will be revised to reach lower socio-economic status adults and depending upon the budget, a general promotion will be developed for free nicotine replacement with coaching.
QUIT@WORK: This employer tool kit was introduced in FY2007 and will be updated as needed.
TobaccoStories.org: this website will be updated to provide more resources, including podcasts, for smokers wishing to quit on their own.
Testimonial Radio: radio spots created from stories of Vermont smokers who have successfully quit using one of Vermont's services. Testimonials will also be posted on TobaccoStories.org.
New Year's Resolutions: media campaign provides smoking cessation tips and resources to smokers thinking about quitting as a New Year's resolution.
Smoking Cessation Promotion (All Adult Smokers)
Objectives: Increase the percentage of quit attempts and increase use of quit smoking resources.
Primary targets: Ages 25 to 44, lower income/lower education
Secondary target: Ages 18 to 24, lower income/lower education
Marketing vehicles: As noted above
Campaign Partners: Community coalitions, Ready. Set…STOP program
Evaluation tools: media reach and frequency, website hits, click rates, materials distribution,
direct mail response, earned media placements, counseling enrollment, ATS.
Media Timing: Fall & Winter 2007-2008
Smoking Cessation (Ages 18 to 24)
The young adult smoking rate (Ages 18 to 24) in Vermont has declined faster than the overall
adult smoking rate, but this group still has a higher smoking rate (27%) than the overall adult rate
(18%).
Young adults are often the target of tobacco industry marketing by direct mail, web promotions,
special magazines and other promotions. Although young adults are not the primary target of this
year's common theme campaign (see Ages 25 to 34), it is important to include messages created
for this group in every annual plan. Last year's television and radio spots, testimonial radio, the
TobaccoStories.org web site and giveaway items will be used again this year to target this age
group.
Smoking Cessation Promotion (Ages 18 to 24)
Objectives
Increase the percentage of quit attempts and increase use of quit smoking resources
Primary Target
Ages 18 to 24, not in college
Secondary Target
Ages 18 to 24, in college
Marketing Vehicles Existing media materials
Campaign Partners Community coalitions, Ready, Set…STOP, state and community colleges
(no required partners for this campaign)
Evaluation Tools
To be determined
Smoking Cessation (Ages 25 to 34): The overall adult smoking rate dropped to 18% in 2006, but the rate for adults between the ages of 25-34 is 22%. This disparity is even larger when looking at lower socio-economic status persons. This age group is the target audience for this year's smoking cessation common theme campaign. Many smokers in this age group have smoked for ten years or more and have tried to quit numerous times. They know how difficult it is to quit. They may even be feel some of the health effects of their habit, and see how it might influence their children. According to the ATS, the vast majority of Vermont smokers want to quit smoking on their own. This year's common theme campaign targets these smokers who do not intend to use the statewide quit smoking services. Every Try Counts redefines quitting smoking as a process, not an event. Quitting smoking takes practice and each quit attempt is part of what many smokers need to do to become smoke-free.
Smoking Cessation (Ages 25 to 34)
Objectives
Increase the percentage of quit attempts and increase use of smoking cessation resources
Primary Target
Ages 25 to 34, lower income/lower education
Secondary Target
Ages 35 to 44, lower income/lower education
Marketing Vehicles Radio spots, talking points for disc jockeys, newspaper insert, classified ad
(Bennington county only), web site updates, free nicotine replacement therapy (NRT) contest, gas station/convenience store advertising and coffee sleeves, giveaways, bar/restaurant coasters, community tools, and statewide and local press releases
Campaign Partners Community Coalitions, Ready, Set…STOP Programs
Evaluation Tools
ATS, measured media, number and duration of community coalition events, media coverage, materials distributed, number of cell phone text-ins to enter contest, visits to TobaccoStories.org, visits to and enrollment in VermontQuitNet.com, calls and fax referrals to counseling, enrollment in counseling
November, December 2007 and January 2008
Smoke-Free Zones
In past years, this common theme campaign focused on creating smoke-free zones around
children. Community partners continued to focus on this objective, but had the option to extend
the message to include adults. In addition, community and hospital partners were encouraged to
promote policy changes with the goal of changing the social norm about the dangers of
secondhand smoke. For example, a number of coalitions identified and worked with local
businesses to create smoke-free zones around business entryways, off-site smoking areas or
smoke-free campuses. Coalitions will continue to work with community members to encourage
smoke-free zones.
Media created for past campaigns were used again. VDH provided resources for community
partners including a campaign brief, giveaway items, campaign images and other downloadable
resources, a press release template and talking points, and idea lists. All of these items were
posted to an extranet site for easy access by partner organizations.
Reduce Exposure of All Vermonters to Secondhand Smoke
Objectives
Increase the awareness that secondhand smoke is harmful in order to increase the proportion of smokers and recent quitters in households with children who ban smoking in the home and car
Primary Target
Parents who smoke, lower income/lower education
Secondary Target
Smokers and recent quitters, lower income/lower education
Marketing Vehicles Radio spots, newspaper insert for southern counties, adult brochure,
children's coloring page, stickers, water bottles, and statewide and local press releases
Campaign Partners Community Coalitions, Ready, Set…STOP Program, Department of
Education, WIC Clinics
Evaluation Tools
Adult Tobacco Survey, distribution of materials, press coverage
August and September 2007
Impact of Media Campaigns
Youth Prevention
Most youth overestimate the percentage of teens that smoke and thus see smoking as a "normal"
teen activity. This misperception about teen smoking leads youth to want to emulate teens. Since
the outset of the Vermont Tobacco Control Program, a major focus of the prevention media
campaigns has been to correct this misperception. The 8 out of 10 common theme campaign was
developed to communicate primarily to middle school youth that 8 out of 10 Vermont teens
choose not to smoke.
According to the 2006 Youth Health Survey (YHS), 44% of middle school students believe
correctly that 8 out of 10 Vermont teens do not smoke cigarettes. This has dropped since 2004,
when 65% of students believed correctly that 8 out of 10 teens did NOT smoke cigarettes. In
addition, 47% of Vermont students have seen a television ad or heard a radio ad that talked about
how many teens choose NOT to smoke. This was down from 70% in 2004. The low number of
students who have seen or heard a specific ad may be due to the timing of the media campaign,
which began after many students had completed the YHS survey.
Smoking Cessation
Findings from the ATS suggest that Vermonters are aware of smoking cessation media
messages. In 2006, 91% of smokers reported awareness of at least one quit smoking
advertisement in the past six months.
The ATS includes questions that can be used to assess confirmed awareness of specific media
campaigns. Respondents are considered to have confirmed awareness of a particular campaign if
they reported having heard or seen campaign ads in the past six months and provided a correct
description of one or more of the campaigns. Confirmed awareness of anti-smoking television
ads rose among all groups from 2004 to 2005 but then dropped in 2006. Confirmed awareness of
at least one of two ads among smokers was 38% in 2005 and 29% in 2006.
Given the high overall awareness of any anti-tobacco media campaign, it is tempting to conclude
the program is reaching most audiences throughout the state. However, the 2004-2006 data for
awareness of specific media messages indicate that this was not the case during the time of year
the survey was conducted, several months after these media campaigns were conducted.
The current appropriation for media and public education in the Vermont Tobacco Control
Program budget is not sufficient to permit sustained promotion of smoking cessation counseling
services throughout the year. The volume of new callers to the Quit Line (and clients enrolling in
Ready, Set.STOP) is highest in the months when the Quit Line is promoted through media
campaigns and direct mail. The volume is lowest in months when mass media promotion is
typically lowest (April through September) unless other types of promotion like direct mail and
news stories occur (Exhibit 24). More sustained systematic promotion throughout the year would
likely result in increased utilization of cessation services, more quit attempts, and fewer
Vermonters smoking.
Exposure to Secondhand Smoke
Less than 10% of the annual funds expended by VDH for media and public education is devoted
to campaigns to reduce the exposure of Vermonters to secondhand smoke. Nonetheless,
Vermont smokers and nonsmokers are changing their behavior. As demonstrated in Section II
under "Exposure to Secondhand Smoke", there is a significant increase in the percentage of
Vermont smokers with children who have policies banning smoking in their homes and vehicles.
According to the RTI, the advent of such voluntary prohibitions on smoking may be an
indication of changes in public awareness of the dangers of secondhand smoke and changing
social norms surrounding exposure to secondhand smoke in Vermont.
Exhibit 24: Current Smoker Calls to Quit Line and Ready, Set…STOP
by Month*, January 2005 - October 2007, New Clients
Quit Line w/o RSS
RSS w/o Quit Line
"Testimonials" -
Mailings - 6/05,
Mailings - 1/07 -
7/06 - 10/06 and
Media: "Money"
Media: "Every Try
Counts" - 11/07 -
"Testimonials"
ENFORCEMENT OF LAWS BANNING TOBACCO SALES TO MINORS
Rationale
As part of a comprehensive program to prevent tobacco use among youth, the Centers for
Disease Control and Prevention (CDC) recommends mobilizing the community to restrict
minors' access to tobacco products combined with additional resources including stronger local
laws directed at retailers, active enforcement of retailer sales laws and retailer education with
reinforcement.
Federal Law
Federal law passed in 1992 requires that all states, as a condition of receiving federal substance
abuse and treatment block grant funds, comply with Section 1926 of the Public Health Services
Act, known as "the Synar Amendment." The stated goal of the law is to reduce illegal purchases
of tobacco by minors. The law sets an 80% compliance goal, or no more than 20% of attempted
purchases by minors resulting in sales, for each state within a negotiated time period. The law
requires the states to do the following: 1) conduct statewide retail compliance checks to ascertain
the prevalence of illegal sales to minors; 2) set an annual goal to reach the 80% compliance rate
through measurable reductions in illegal sales and continuation of reductions; and 3) report the
results annually to the federal government. Vermont has exceeded the 80% compliance rate
since 2001.
Vermont Law
In 1997, Vermont set a higher standard: 90% compliance. Vermont law (Act 58) directs the
Department of Liquor Control (DLC) to conduct "compliance tests of tobacco licensees as
frequently and as comprehensively as necessary to assure consistent statewide compliance with
the prohibition on sales to minors of at least 90% for 17-year old buyers." Vermont is the only
state to have raised the standard above the 80% federal level, although several states have
achieved compliance rates of 90%. Vermont is the only state that requires that only 17-year-old
youth participate in compliance checks. Some states allow youth as young as 14-years-old, but
most have teens ages 16 and 17 serve as their buyers in the compliance checks. There is some
research indicating that the younger the appearance of the youth who attempts to buy cigarettes
in the compliance check, the fewer the number of illegal sales.
In 2002, the Legislature made training mandatory for tobacco licensees and sellers. Prior to July
2002, the DLC chose to include tobacco training in the mandatory training it conducted for
alcohol licensees and servers. In 2002, the Legislature also amended the statute to lower the
penalties to retailers that failed tobacco compliance checks, imposing a warning for a first
failure.
Independent Evaluation: Vermont's Retailer Compliance Rate
Since 1999, Vermont has not achieved the 90% tobacco retailer compliance rate required by Act
58. As detailed in the board's 2007 annual report, RTI, the independent program evaluation
contractor, evaluated the state's program to restrict minors' access to tobacco products,
compared Vermont's program with those of other states, and made recommendations for
achieving at least 90% compliance. RTI concluded the following:6
Enforcement inspections are essential to maintain high compliance rates. Key factors in the effectiveness of such inspections include: age of buyer, age of seller, whether the
6 Farrelly et al, RTI International, Assessing Vermont's Program to Restrict Youth Access to Tobacco Products, April 2006.
buyer knows the seller, and attitude and demeanor of the buyer. Other techniques needed to maintain compliance above 80% include effective merchant education and penalties for violations.
As enforcement becomes more effective, some minors will shift from commercial to social sources to obtain tobacco. Increasing compliance rates without addressing alternative commercial and social sources for tobacco may not result in a true reduction of youth access. In 2006, 89% of Vermont high school students who smoked reported obtaining cigarettes by "borrowing" from a friend or family member, stealing, or giving money to someone to purchase.
RTI identified and analyzed three main options for improving Vermont's rates of compliance:
1. Increase the number of annual compliance checks; 2. Increase the number of retail clerks trained directly by Department of Liquor Control; 3. Increase penalties for noncompliance.
According to RTI, each of the options above has evidence to suggest it would lead to increased retailer compliance. RTI recommended Option 3 (increasing the penalties for noncompliance) as the most cost-effective option. Vermont law provides for a warning to a retail licensee upon the first failed compliance check; this is more lenient than other high-compliance states. Option 1 (increasing the number of compliance checks conducted) and Option 2 (increasing the number of DLC-provided training sessions) are the most costly options presented in this study, and the improvements in retailer compliance from these options may not be significant enough to merit the expenses incurred. The literature and data for other states suggests that the penalties for noncompliance with youth access laws appear to be one of the most important determinants of compliance rates.
The Enforcement Committee met in May 2007 to evaluate recent information regarding youth smoking and retail compliance rates, and to develop a recommendation to the board. The committee heard and discussed legislative developments, data on retailer compliance and youth smoking, research and analysis regarding the effectiveness and cost effectiveness of various control methods, and the results of recent focus groups regarding youth access to tobacco. As a result, the board adopted two resolutions, recommended by the Enforcement Committee, at its May 16th meeting. They are:
1. To address youth access to tobacco through social sources in Vermont's tobacco
prevention and control efforts. Implementation measures:
• integrate education across the relevant components to send the message to communities
and teens that providing cigarettes to minors is illegal.
• study fines for furnishing to a minor (already in existence in Vermont statue). • study enforcement methods used to enforce prohibitions on supplying tobacco to kids
(e.g., shoulder taps) in other states.
2. To continue Vermont's enforcement program to prevent retail sales of tobacco to
minors, and develop and support evidence-based means of further improving retail
compliance rates. Implementation measures:
• Support increase of approximately $90,000 of tobacco settlement funds to be
appropriated for a new tobacco-only DLC investigator position.
• Continue to support H.149, to provide for retail tobacco licenses to be issued by DLC,
thus improving the DLC database of current tobacco licensees.
• Publicize compliance check results at the local level through community coalitions. • DLC should develop information and report on the potential for requiring retail clerks
selling tobacco (and alcohol) to obtain sellers' licenses from DLC.
• DLC and the Attorney General's Office should work with DMV to evaluate potential
improvements to Vermont Identification Cards to more easily distinguish youth under the legal age for tobacco purchases.
Tobacco Licensing
Tobacco licenses are currently issued by the local town or city, with the proviso that they should
report the issuance or expiration of any tobacco license to the DLC. This system results in the
DLC having outdated information in their tobacco license registry. Thus, the DLC incurs
excessive costs in their unannounced compliance checks by attempting checks on businesses that
no longer sell tobacco or have closed. RTI recommended the DLC should have the sole authority
for issuing tobacco licenses. According to RTI, this would improve the accuracy of the database
of tobacco retailers maintained by DLC and would reduce some of the confusion and efficiency
losses currently incurred by having tobacco-only licenses issued through municipalities. The
town will not lose its control of the application of tobacco and alcohol licensing or any
associated fees.
Compliance Checks
The Department of Liquor Control submits an annual report to the Legislature on its compliance
program for alcohol and tobacco sales. The key findings regarding tobacco control relate to the
number of tobacco compliance checks conducted with licensees and the rate of compliance
(Exhibit 25). An increase in compliance checks by Department of Liquor Control in 2004 led to
an increase of compliance rates but did not achieve the required 90% level. Vermont has one of
the highest rates of retailer compliance checks among the states. RTI has pointed out that
Vermont's use of 17-year-old checkers is a more intensive check of compliance than other states.
EXHIBIT 25: Rate of Compliance with Tobacco Sales Laws among Licensees Checked,
Calendar Years 2000-2007 and FY2006 and 2007
DLC Compliance Checks, 2000-2007
Retailer Training
The DLC trains over a thousand retail employees each year at seminars that address the laws for
alcohol and tobacco licensees. A small percentage of these seminars were co-sponsored by
community tobacco coalitions, which took responsibility for logistics, recruitment of attendees,
and refreshments. Most of the time allocated in training seminars is directed toward
alcohol-related laws.
Exhibit 26: Level of Training of Retail Clerks Who Passed and Who Failed Tobacco Compliance Checks, Calendar Year 2007
Level of Clerk
Number of
Compliancy
Training
(did not sell)
Clerk trained by DLC
Clerk trained by retailer
Clerk not trained
As noted in Exhibit 26, clerks trained by the DLC have a significantly higher rate of compliance
with the law (92.1%) than clerks who are trained by their employers (82.6%) or are not yet
trained (71.7%). Although it appears that the DLC-provided training is more effective than
retailer-provided training at promoting compliance, the RTI report noted that the differences in
compliance rate of DLC-trained clerks might be driven by underlying differences between
retailers. Those retailers who are more willing to make serious efforts to comply with the law
may also have been more likely to request the DLC-provided training.
Consideration of Increased Penalties
The RTI report recommended that Vermont increase its penalty structure for sales to minors, to
bring it into alignment with other high-compliance states. After the Vermont Legislature revised
the penalty structure in 2002 to provide for a warning for a first offense, fines to retailers
decreased and there were very few suspensions of tobacco retailers' licenses. Vermont currently
has one of the most lenient penalty structures for tobacco youth access violations. RTI concluded
that the state's compliance rates would likely increase if retailers were fined for the first offense.
The board has accordingly recommended further analysis of this issue and the Enforcement
Committee will continue its review.
Internet Sales of Tobacco Products
According to the 2006 Youth Health Survey, 5% of smokers in grades 8-12 purchased cigarettes
on the internet in the last 12 months. According to the Vermont Adult Tobacco Survey, 33% of
adult smokers reported they purchased some cigarettes and 1.1% of adult smokers purchased at
least 25% of their cigarettes on the internet in the past 12 months. In its 2007 report, Ending the
Tobacco Problem, A Blueprint for the Nation, the Institute of Medicine stated the only practical
way to effectively regulate online tobacco retailers is through legislation prohibiting both online
tobacco sales and shipment of tobacco products directly to consumers. The board recommends a
complete ban on the sale of tobacco products through delivery methods including the internet,
telephone and mail order in an effort to further reduce youth access to tobacco products.
IV. ROLE OF THE BOARD
RESPONSIBILITIES
The legislation that created the Vermont Tobacco Evaluation & Review Board requires the board
to meet at least quarterly. However, the board tries to meet monthly. The full board met in
person nine times and twice by conference call in 2007. In addition, each of the five standing
committees meets as necessary. The greatest workload is undertaken by the Evaluation
Committee. It meets frequently to review numerous draft documents and data that are the basis
for assessing program activities and outcomes. All five committees – community and schools,
cessation, enforcement, evaluation and media and public education – convened throughout the
summer as each considered program and budget recommendations for FY2009. See Section VII,
Appendices for the list of board members, with the criteria for appointment and term of office.
The responsibilities of this board, as detailed in the legislation, are substantial. They are listed
below along with a brief summary of the board's activities in 2007 to fulfill those
responsibilities. Details about the board's activities are provided throughout this report.
ACTIONS IN 2007
Evaluation
The board selects and oversees the work of the independent evaluation contractor.
The board selected, through a competitive bid process, Research Triangle Institute (RTI) for the
initial contract for independent evaluation that commenced in February 2002 and for the current
contract, which began in January 2005. Since the board has the responsibility for overseeing the
work of the contractor and the Department of Health (VDH) has responsibility for entering into
the contract with RTI, the management structure initially presented some challenges. However,
the three organizations have over time successfully addressed differences in priorities and
timelines to reach consensus on work specifications and tasks. Much of the data included in this
annual report is the product of RTI's work. The Evaluation Committee has been vigilant in
reviewing draft documents, as has the VDH staff in the Health Surveillance Division and the
coordinator of the Department of Education's (DOE) tobacco prevention program. The
Department of Liquor Control (DLC) has provided considerable data to RTI regarding the
tobacco compliance checks conducted in Vermont, as well as the penalties and suspensions
imposed for sale of tobacco to minors.
The current evaluation contract expires on June 30, 2008. A request for proposals (RFP) will be
issued at the end of February 2008 for a two-year contract with the option of renewal for another
two years. The Evaluation Committee reviewed and approved the proposed work specifications
in December 2007. The full board will vote on the recommendations of the evaluation committee
at its January 2008 meeting.
Program Work Plan
The board, in collaboration with the Department of Health, is required to prepare an annual
plan, with goals for each component of the program, by June 1st
The administrator of the Tobacco Evaluation and Review Board developed the annual program
objectives in the spring of 2007 in collaboration with the Departments of Health, Education and
the Liquor Control. The Vermont 2008 & 2009 Tobacco Control Workplan was released in the
fall of 2007.
Public Meetings
The board is required to hold at least two public meetings by September 15th of each year to
receive public input for setting program priorities and budget.
On June 20 2007, the board hosted a public meeting through Vermont Interactive Television
(VIT). The public could participate in Bennington, Brattleboro, Johnson, Lyndonville,
Middlebury, Rutland, St. Albans, Waterbury (host site) and Williston. Ten people testified and
four sent emails prior to the hearing. As noted in the board's 2007 report, since 2001, public
meetings have been poorly attended. The board has looked for new and creative ways to start the
public conversation. In July 2007, the board's proposed FY2009 program and budget
recommendations were posted to the board's website at www.humanservices.gov/tobacco to give
stakeholders the opportunity to comment via email, letter or fax.
Annual Budget
By October 1st of each year, the board submits an independent budget recommendation for the
tobacco control program to the Governor and Legislature.
The board recommendation for the FY2009 budget for the Vermont Tobacco Control Program
calls for an increase of $3.2 million for a total of $ 8,452,604. Most of the increase is directed
toward adult smoking cessation services. An overview of the recommendation appears in
Section V, Tobacco Evaluation and Review Board Recommendations of this report.
Community-based Programs
The board collaborates with the Department of Health in defining the criteria for rating
community coalition grant applications; and the board reviews each grant application and
provides funding recommendations to the Commissioner of Health.
As of FY2007, the tobacco community coalition grants may be renewed for one additional year
subject to the availability of funds. All grants were renewed in FY2008. The Community and
School Programs Committee reviewed and approved the FY2009 work specifications in
September 2007 and the board voted on the committee's recommendation in October. The board
will begin to review FY2009 applications in March 2008.
School-based Programs
The board reviews and makes recommendations regarding the school-based activities funded by
the tobacco control program.
The board's independent evaluator, RTI, worked with the Department of Education tobacco use
prevention program coordinator to develop a survey for school-based tobacco prevention
coordinators. Coordinators completed the survey at the annual statewide tobacco control partners
meeting in September 2007. RTI is preparing a report that will inform the board on future
tobacco use prevention curricula implementation recommendations.
Media and Public Education
The board must approve all media campaigns.
The board is responsible for selecting, upon the advice of the Commissioner of Health, the
contractor responsible for countermarketing campaigns and public education. The board in
concurrence with the recommendation of the Commissioner of Health, voted to select Kelliher
Samets Volk for the media and public education contract of approximately $1 million for
FY2007, renewable for up to two years.
The process agreed upon by the board and the Department of Health for securing board approval
of media campaigns involves the following steps: 1) the Media & Public Education Committee
first reviews the creative work plan for the new campaign, which details the objectives, the target
group, the strategy for reaching them, the messages and media to be used; 2) the creative work
plan, or a revised version thereof, is presented to the full board at which time the committee chair
presents the recommendation of the committee and their rationale for it; 3) rough ads are created
and shown to the Media & Public Education Committee; and 4) the ads, revised if necessary, are
presented to the full board for action on the committee's recommendation.
In February 2007, the board approved the media campaign called The Butts of Hollywood. This
goal of the campaign was to increase media literacy by motivating teens to think critically about
smoking portrayed in movies and to take action. In October 2007, the board approved Every Try
Counts designed to remind smokers that quitting is a process, not an event. The target group was
25-34 year-olds and the campaign attempted to reach smokers when and where they were likely
to smoke.
Enforcement
The board reviews and makes recommendations to the Department of Liquor Control regarding
their activities to ensure compliance with state law regarding tobacco sales to minors.
DLC is charged with enforcement of state laws prohibiting sales of tobacco products to minors.
In 1997 the Legislature enacted Act 58, requiring DLC to conduct or contract for compliance
testing "as necessary to assure consistent statewide compliance with the prohibition on sales to
minors of at least 90 percent for 17-year-old buyers."
Since 1999, Vermont has not achieved the 90% tobacco retailer compliance rate required by Act
58. In May 2007, the board adopted a resolution to continue Vermont's enforcement program to
prevent retail sales of tobacco to minors, and develop and support evidence-based means of
further improving retail compliance rates. See Section III, page XX for implementation
measures.
Coordination
The legislation calls for the board to propose to the Department of Health strategies for program
coordination and collaboration across state agencies, nonprofit organizations, health providers,
and other anti-tobacco groups.
The board was the catalyst for several efforts to increase the coordination across the components
of the comprehensive tobacco control program and enhance the collaboration among the
Departments of Health, Education, and Liquor Control. These efforts by the board were
described in the board's 2005 and 2006 Annual Reports.
Over 120 tobacco control grantees, contractors, state agencies, and stakeholders participated in
the statewide tobacco control partners meeting on September 25, 2007 in Rutland. This annual
meeting provides time to discuss shared work, expand on work plan objectives and improve
collaboration. The primary topic areas this year were improving access to smoking cessation
resources for adults and reducing social sources of tobacco for youth.
VDH convened a Scientific Advisory Panel, at the request of the board's Cessation Committee,
to make recommendations to improve coordination of Vermont's smoking cessation services.
VDH and the board will review the panel's recommendations in the winter of 2008 and VDH
will make a final set of determinations about coordinating these programs by the end of FY2008.
Annual Report
By January 15th of each year, the board is required to submit to the Governor and the
Legislature a report that addresses the following: board's activities, financial reports of the
board and the three departments, recommended program budget, explanation of outcomes of
programs, and (beginning with the 2003 report) the results of the independent program
evaluation.
V. TOBACCO EVALUATION AND REVIEW BOARD
LEGISLATION: FY2009 APPROPRIATIONS
Increase Funding for the Tobacco Control Program
The board recommends an increase of $3.2 million for a total of $8.4 million in program funds
for FY2009 to address areas – in particular adult smoking cessation - that need to be
strengthened in order to remain on course with the anticipated program outcomes. Investment in
the state's comprehensive tobacco control program is critical to improving the health and
reducing health care costs of all Vermonters.
In October 2007, the Centers for Disease Control and Prevention (CDC) updated its 1999 Best
Practices for Comprehensive Tobacco Control Programs. It recommends that Vermont spend
$10.4 million on the statewide comprehensive tobacco control program. According to the CDC,
research shows that the more states spend on comprehensive tobacco control programs, the
greater the reduction in smoking. The longer states invest in such programs, the greater and
faster the impact. States that invest more fully in comprehensive tobacco control programs have
seen cigarette sales drop more than twice as much as in the United States as a whole, and
smoking prevalence among adults and youth has declined faster as spending for tobacco control
programs has increased. See pages 54-56 for the board's FY2009 program and budget
recommendations.
Allocate Funding to the Tobacco Trust Fund
The board recommends that money from the annual Master Settlement Agreement (MSA) should
be appropriated to the Tobacco Trust Fund to develop a long-term sustainable source of support
for the tobacco control program that is not dependent on the tobacco industry. This is in
accordance with the recommendation by the Vermont Tobacco Task Force, created by the
Legislature and the Governor in 1999 and charged with developing a comprehensive plan for use
of the MSA funds.
LEGISLATION: 2008
Support H.149 to:
Give the Department of Liquor Control (DLC) the ability to issue each retail
tobacco license. Tobacco licenses are currently issued by the local town or city, with the
proviso that they should report the issuance or expiration of any tobacco license to the
DLC. This system results in the DLC having outdated information in their tobacco
license registry. Thus, DLC incurs excessive costs in their unannounced compliance
checks by attempting checks on businesses that no longer sell tobacco or have closed.
The town will not lose its control of the application of tobacco and alcohol licensing or
any associated fees.
Impose a Minimum Age to Sell Tobacco. There is currently no statute setting a
minimum age to sell tobacco in Vermont. Research has consistently demonstrated that
the younger the seller of tobacco, the greater the likelihood of an illegal sale to a minor.
The board recommends that the minimum age to sell tobacco is 16 years of age.
H.149 passed the House of Representatives in March 2007 and is currently in Senate Economic Development, Housing and General Affairs.
Support ban of home delivery sales of tobacco products
According to the 2006 Youth Health Survey, 5% of smokers in grades 8-12 purchased cigarettes
on the internet in the last 12 months. According the 2006 Vermont Adult Tobacco Survey, 33%
of adult smokers purchased some cigarettes and 1.1% of adult smokers purchased at least 25% of
their cigarettes on the internet in the past 12 months. In its 2007 report, Ending the Tobacco
Problem, A Blueprint for the Nation, the Institute of Medicine stated the only practical way to
effectively regulate online tobacco retailers is through legislation prohibiting both online tobacco
sales and shipment of tobacco products directly to consumers. The board recommends a
complete ban on the sale of tobacco products through delivery methods including the internet,
telephone and mail order in an effort to further reduce youth access to tobacco products.
Shift term expiration date of Tobacco Evaluation and Review Board members from
February 1 to July 1. Currently board member terms begin February 1 (Title 18, Chapter 225,
§9504(b), during the legislative session and one month prior to the community coalition grant
application review. This current system is a challenge for new members, the board chair and the
administrator. Shifting the date to July 1 would allow for a smoother transition.
ADDITIONAL RECOMMENDATIONS
Develop model legislation for a complete ban of smoking in all Vermont workplaces. There
is an exception in the Smoking in the Workplace Law (Title 18, Chapter 28, §1422 – 1424) that
allows smoking in designated unenclosed smoking areas. The board recommends developing
model legislation to provide a smoke-free workplace for all Vermont employees.
Develop smoke-free multi-unit housing residences, both existing and planned. In the 2006
report, The Health Consequences of Involuntary Exposure to Tobacco Smoke, the U.S. Surgeon
General concluded the scientific evidence indicates there is no risk-free level of exposure to
secondhand smoke. The board recommends developing smoke-free policies to reduce exposure
of secondhand smoke for Vermonters living in multi-unit housing.

Vermont Tobacco Evaluation and Review Board
Vermont Agency of Human Services � 103 South Main Street � Waterbury, VT 05671-0203
Tel: 802-241-2555 � Fax: 802-241-4461 � Email: [email protected]
TO: The Honorable Governor James Douglas
Senate Appropriations Committee
Theodore Marcy, MD, MPH
House Appropriations Committee
Joint Fiscal Committee
Brian S. Flynn, ScD
FROM: Theodore Marcy, MD, MPH, Chair
Vice Chair
DATE: October 1, 2007
Representative Patsy French
RE: FY2009 Budget Recommendation for the Tobacco Control Program
(Section 271 of Act 152 (2000), 18 V.S.A. chapter 225, s.9505(9))
Senator Sara Kittell
Tobacco use continues to be the number one cause of preventable death, costing
Vermont $233 million per year in health care, $66 million of which are Medicaid
expenditures. Investment in the state's comprehensive tobacco control program is
Gregory MacDonald, MD
critical to improving health and reducing health care costs of all Vermonters. The
board recommends an FY2009 budget of $8,452,604 for the tobacco control
program. This is an increase of $3,227,657 from FY2008.
Edna Fairbanks Williams
Our recommendation is similar to what Vermonters told the Tobacco Task Force
in 1999 when this task force was charged with developing a comprehensive plan
Ex Officio
for use of the funds from the Master Settlement Agreement (MSA). Vermonters
Attorney General
across the state overwhelming wanted to invest these funds in comprehensive
statewide tobacco prevention and cessation programs: 1/3 for tobacco control
Commissioner of Education
programs, 1/3 for a tobacco trust fund, and 1/3 for tobacco-related health needs.
The Legislature responded and passed laws to create and fund a comprehensive
statewide tobacco control program. Since 2001, however, Vermont has
Commissioner of Health
appropriated a majority of the annual payment to Medicaid and a small portion to
Sharon Moffatt, Acting
the tobacco control program. In the current fiscal year for example, only 12% is
Commissioner of Liquor
directed to the tobacco control program. The board's recommendation is just
under 25% of the anticipated $37 million of the FY2009 MSA payment.
The decrease in Vermont's adult smoking rate to 18% in 2006 is encouraging
evidence that Vermont's comprehensive tobacco control program, smoke free
workplace laws, and tobacco tax increases can have a positive impact. However,
Administrator
the state will not reach its goal of reducing the adult smoking rate to 11% by 2010. There are still 88,000 adults who smoke including 30% of low-income Vermonters, and 44% of those with moderate or severe depression. In order to help smokers quit, especially those disparately impacted by tobacco use, Vermont should expand and enhance its smoking cessation and tobacco control programs as outlined in the attached program and budget recommendations. Thank you for your consideration of these requests. Please let me know if you would like additional information.
FY08 Budget
FY 09 Recommend Exhibit 27: Vermont Tobacco Evaluation and Review Board FY2009 Budget Recommendation
(increase)
Department of Health
$1,400,211
$2,173,484
Tobacco Cessation Programs - Helping Smokers Quit:
(+$773,273)
Increase Access to Nicotine Replacement Therapy ($500,000): Smokers who use nicotine replacement
therapy (NRT) to help them quit have twice the success rate of smokers who do not use NRT. The FY08
budget is $315,000 and more funding is needed to provide free NRT to smokers ready to quit.
Increase Access to Quit Smoking Services ($500,000): The adult smoking rate in Vermont was 18% in 2006.
However, there are special populations of Vermonters with higher smoking rates including pregnant women
(19.7%), low income (30%) and people with moderate or severe depression (44%). Funding would be allocated
to mental health & substance abuse centers, Federally Qualified Health Centers, Vermont Clinics for the
Uninsured, WIC clinics and ScoreHealth to refer clients to the free quit smoking programs.
Quit Smoking Programs ($1,173,484): To continue free quit smoking programs including hospital-based
counseling ($759,084), phone counseling ($250,000), web-based support ($52,500) and N-O-T teen quit
smoking program ($111,900).
$1,023,624
$1,626,860
Community-based Programs:
(+603,236)
Community Coalitions ($1,103,328): To fill gaps in community tobacco coalitions' service areas.
Approximately 134,000 Vermonters do not have access to community coalition support and activities.
CHAMPPS ($100,000): To award grants for community health and wellness projects, specific to tobacco
control, as established by the Legislature in 2006.
Youth and Young Adult Prevention ($180,000): To award grants to Our Voices Exposed (OVX), Vermont
Kids Against Tobacco (VKAT) and colleges to mobilize youth and young adults to serve as role models and to
persuade peers to remain tobacco free.
Community Training, Development and Staff ($243,532): To increase district office prevention consultants
from 10 to 12 ($143,532) and dedicate 10% of each consultant's time to technical support for local tobacco
control efforts. To increase leadership and disparity training ($100,000) for those working in community
tobacco control.
$1,007,799
$1,925,500
Media & Public Education:
(+$917,701)
Preventing Youth from Starting to Smoke ($775,500): To develop and implement media campaigns
targeting youth between the ages of 10-13 and 14-17 in the same year. The current budget allows for emphasis
on one age only group per year.
Helping Smokers to Quit ($990,000): To increase awareness of free quit smoking resources including phone
and hospital counseling, online support and NRT. To provide resources and tools for the majority of smokers
who prefer to quit on their own.
Reducing Exposure to Secondhand Smoke ($100,000): To provide additional media and campaign materials
to increase the percentage of Vermont adult smokers who prohibit smoking in their homes and cars.
Contingency Planning ($60,000): To allow for consumer insight research for campaign planning and
unexpected opportunities.
FY08 Budget
FY 09 Recommend Exhibit 27 (cont): Vermont Tobacco Evaluation and Review Board FY2009 Budget Recommendation
(increase)
Department of Health (continued)
$200,000
Statewide Provider Education: To expand the current pilot program to healthcare providers to:
(+$125,000)
educate them about Vermont's free quit smoking services.
establish office systems to identify smoking status of each patient at every visit.
give free NRT to patients who smoke and choose to quit on their own.
$333,000
$766,309
Surveillance and Evaluation:
(+433,309)
Focus Group ($50,000) and Adult Longitudinal Survey ($100,000): To understand why or why not smokers
choose group counseling. To develop new methods to increase quit attempts and treatment seeking.
Media Tracking ($150,000): To better understand media penetration by conducting surveys in waves
proximate to media campaigns.
Full-time Data Analyst ($88,000): To provide increased data collection and analysis for new programs.
Adult Tobacco Survey (ATS) ($125,000): To continue annual telephone survey of smokers and
non-smokers.
Hospital Counseling Data ($30,000): To continue hospital-based counseling program data collection.
Independent Evaluation Contract ($223,309): To continue independent program evaluation as mandated by
Vermont statute.
$3,839,634
$6,692,153
Total: Department of Health
Department of Education
$995,668
$1,255,668
Distance Learning and Support for Health Educator Licensure ($200,000): To increase the number of
(+$260,000)
educators with a health education certification to deliver health education programs including tobacco
prevention.
Alcohol, Tobacco and Other Drug (ATOD) training ($50,000): To train staff to build knowledge and skills
for ATOD prevention per Act 51 requirement.
Prevention collaborator's conference: ($10,000): To create an annual meeting for school-based prevention
educators and collaborators.
Supervisory union grants and technical assistance ($989,007): To continue grants and technical assistance
to supervisory unions to implement model tobacco prevention programs.
Governor's Youth Leadership Conference ($6661): To continue to implement tobacco track.
FY08 Budget
FY 09 Recommend Exhibit 27 (cont): Vermont Tobacco Evaluation and Review Board FY2009 Budget Recommendation
(increase)
Department of Liquor Control
$289,645
$379,783
Expand Enforcement Oversight ($90,138): To fund a full-time tobacco only investigator to enable DLC to
(+90,138)
expand its enforcement to:
conduct regular inspections of retail tobacco licensees and wholesalers for compliance including fire-safe cigarettes, tax stamps and clean indoor air law.
investigate smuggling of cigarettes and tobacco products.
perform compliance checks regarding sales by internet cigarette and tobacco sellers.
work special details at schools and problem areas to enforce youth tobacco laws.
assist in recruiting minors for compliance checks.
address other tobacco-related enforcement issues as they arise.
Retailer Training and Compliance Checks ($289,645): To continue training retail tobacco licensees and their
employees and implement compliance checks for underage tobacco sales as required by statute.
Tobacco Evaluation and Review Board (Agency of Human Services)
$100,000
$125,000
Youth Access Analysis ($25,000): When the Legislature created the board in 2000; it granted it the ability to
(+25,000)
employ technical experts as needed. The board needs technical expertise to:
address social sources (family, friends, etc) of tobacco products for minors.
develop a plan to integrate reduction of youth access to tobacco products through social sources into Vermont's tobacco control and prevention efforts.
Board Support ($100,000): To continue funding one full-time staff, administrative support, benefits,
meetings, materials, supplies, staff and board member travel, board member per diem, etc. as directed by
statute.
$5,224,947
$8,452,604
Total: Tobacco Control Program
VI. FINANCIAL REPORTS
The board is required to include in its annual report "a full financial report of the activities of the departments of health, education, liquor control, and the board, including a special accounting of all activities from July 1 through December 31 of the year preceding the legislative session during which the report is submitted."
Exhibit 28: Vermont Tobacco Evaluation & Review Board
Expenditures, July 1, 2007-December 31, 2007
Appropriation - FY2008
$100,000.00
Board: Meeting Refreshments
Board: National Conference on Tobacco or Health (Presenter)
Board: Online course – Program Evaluation
Advertising (Public Notices)
Telephone & Conference Calls
Vermont Interactive Television (Public Meeting)
Postage and Shipping
Equipment (LCD projector)
Board Service Acknowledgment
Administrative Support
Administrator: Salary & Benefits
Administrator: Instate Travel
Administrator: National Conference on Tobacco or Health (Presenter)
Administrator: American Public Health Association Meeting
Administrator: Out-of-state meeting (FY07)
Administrator: Online course, Program Evaluation
Total (first half of FY2008):
44,285.62
Balance FY2008:
55,714.38
Exhibit 29: Vermont Department of Health
Tobacco Control Expenditures, July - December 2007
Health Disparities Grant
Tobacco Settlement
TOTAL - all programs
DETAIL BY PROGRAM
$638,739.00
Health Disparities Grant
Tobacco Community-Based
$904,059.00
Tobacco Countermarketing
$237,841.00
Tobacco Cessation
$904,565.00
Tobacco Surveillance &
$52,912.00
TOTAL - all programs
CDC= Centers for Disease Control and Prevention
ALF= American Legacy Foundation
MSA= Master Settlement Agreement
Exhibit 30: Department of Liquor Control Settlement Funds
Expenditures, July 1, 2007-December 31, 2007
Appropriation - FY2008
$289,645.00
Education:
Personnel Services
Operating Expenses
$130,864.65
Tobacco Compliance:
Personnel Services
Operating Expenses
$20,558.92
Total (first half of FY2008):
151,423.57
Balance FY2008:
$138,221.43
Exhibit 31: Tobacco Litigation Financial Report
Submitted by the Department of Education, December 31, 2007
This is the financial report for the Tobacco Litigation Settlement money from the Department of Education. The Program Manager
and Director expect to fully expend this year's appropriation. There may be some grant money returned as the last year's final
reports come in from the LEAs. It is not expected that this amount will be substantial.
Personal Services FY2008
Projected Expenditures Total Projected Expenses
12/01/07-6/30/08
Description
Salary & Wages - Overtime
Health Insurance
Dental Insurance
Employee Assistance Program
Worker's Comp. Insurance Premium
Contracted Services - Education/Training
$53,929.88
480,726.52
$134,656.40
Operating Expenses FY2008
7/1/07 - 11/30/07
Buildings and Land - Other than Office Space
Equipment and Vehicles
General Liability Insurance Premium
Telecommunications - Telephone Service
IT Internal Services Cost - DII - Other
IT Internal Services Cost - VISION Assessment
IT Internal Services Cost - Telephone
Printing and Binding
Process & Printing Films, Microfilm
Freight and Express Mail
Instate Conference, Meetings, etc.
Other Purchased Services
Other General Supplies - Educational
Books & Periodicals - Library/Educational
Hardware - Office Desktop & Laptop PC's
Software - Office Technology
Other Equipment - Office
6,412.95
23,940.09
30,353.04
Grants FY2008
Projected Expenditures Total Projected Expenses
7/1/07 – 11/30/07
12/31/07 – 6/30/08
550020 Grants to School Districts
550200 Grants, Awards, Scholarships and Loans
550500 Other Grants
162,451.10
666,625.90
829,077.00
APPENDICES
APPENDIX 1
Vermont Tobacco Evaluation & Review Board: Members and Terms of Office
APPENDIX 2
Vermont Tobacco Control Budget Recommendation: Best Practices for Comprehensive Tobacco Control
Programs, the Centers for Disease Control and Prevention, October 2007
APPENDIX 3
Smoking Rates in Vermont, By Age and Specific Populations
APPENDIX 4
Our Voices Exposed (OVX) and Vermont Kids Against Tobacco (VKAT) grants
VERMONT TOBACCO EVALUATION & REVIEW BOARD MEMBERS
Appointed Members
Appointment Criteria and Term
Chair, 2006 – 2008
Tobacco Use Researcher
Theodore Marcy, MD, MPH
Appointed by the Governor
Term expires: 2010
Vice Chair, 2006-2008
Countermarketing Expert
Brian Flynn, ScD
Appointed by the Governor
Term expires: 2008
Amy Brewer, MPH
Non-profit Anti-tobacco Organization
Appointed by the Speaker of the House Term expires: 2009
Representative Patsy French
Vermont House of Representatives
Appointed by the Speaker of the House Term expires: 2009
Senator Sara Kittell
Vermont Senate Appointed by the Senate Committee on Committees Term expired: 2010
Coleen Krauss
Educator (K-12) - Prevention Education
Appointed by the Governor Term expires: 2008
Ryan Krushenick
Person Under Age 30
Appointed by the Speaker of the House Term expires: 2009
Gregory MacDonald, MD
Health Care Community Representative
Appointed by the Governor Term expires: 2009
Erica Peters
Person Under Age 30
Appointed by Senate Committee on Committees Term expires: 2009
Edna Fairbanks Williams
Low Income Community Representative
Appointed by the Senate Committee on Committees Term expires: 2008
Ex Officio Members
Richard Cate
Commissioner, Department of Education
Michael J. Hogan
Commissioner, Department of Liquor Control
Sharon Moffatt
Acting Commissioner, Department of Health
William Sorrell
Vermont Attorney General
Designees for Ex Officio Members
Sheri Lynn
Designated by the Commissioner of Health
Tobacco Control Chief
Christy Taylor Mihaly
Designated by the Attorney General
Assistant Attorney General
Kate O'Neill, Coordinator
Designated by the Commissioner of Education
Student Health & Learning
Staff
Rebecca L. Ryan, MEd., Administrator
Vermont Tobacco Evaluation and Review Board
Agency of Human Services, Office of the Secretary
103 South Main Street, Waterbury, VT 05671-0201
[email protected]; 241-2555
Smoking Rates in Vermont
Adult Smoking Rates, By Age7
All: 18+ Smokers
Smoking Rates for Specific Populations
Most recent data
Adults living below 125% of Federal Poverty Limit (FPL)
Moderate or severe depression (past 14 days)
Youth Smoking Rates, By Grade11
Year
7 Behavioral Risk Factor Surveillance Survey (BRFSS, 2001-2006) 8 BRFSS, 2006 9 Vermont Birth Certificate Data, 2004 10 BRFSS, 2006 11 Youth Risk Behavioral Survey
Appendix 4 Vermont Kids Against Tobacco (VKAT) Sites by County (CDC funds), FY2008
VKAT Sites
Grant FY2008
Addison County
Middlebury Union Middle School
Orwell Village School
Vergennes Middle School
Bennington County
Arlington Memorial High School
Caledonia County
Lyndon Town School
Peacham Elementary School
St. Johnsbury School
Waterford School
Chittenden County
Albert D. Lawton School
Brown's River Middle School
Camel's Hump Middle School
Edmunds Middle School
Frederick H. Tuttle Middle School
Hinesburg Community School
Lyman C Hunt Middle School
Mater Christi School
Milton Elementary School
Williston Central School
Winooski Middle School
Essex County
Franklin County and Grand Isle County
Berkshire Elementary
Enosburg Falls Middle School
Fairfield Central School
Franklin Central School
Grand Isle School
Montgomery Elementary School
Richford Elementary School
Sheldon Elementary School
Swanton Central School
Orleans County
Albany Community School
Craftsbury Academy
Holland Elementary School
Rutland County
VKAT Sites
Grant FY2008
Benson Village School
Boys and Girls Club of Rutland County
Castleton Village School
Fair Haven Grade School
Mount Holly Elementary School
Proctor Junior High
Washington County
Central Vermont New Directions
Northfield Middle and High School
Windham County School
The Collaborative
Twin Valley Middle School
Windsor County
Ludlow Elementary School
Riverside Middle School
Rochester School
Windsor Middle School
Woodstock Union Middle School
Total VKAT Grants
Our Voices Xposed (OVX) Sites by County*, FY2008 (CDC funds) * Some grantees serve town(s) in additional counties
OVX Sites
GRANT FY2008
Addison County
Middlebury Union High School
Bennington County
The Collaborative
Chittenden County
Mount Mansfield Union High School
Burlington High School
Rutland County
Boys and Girls Club of Rutland
Washington County
Central Vermont New Directions
New Directions for Barre
Windsor County
Black River Area Community Coalition
Rochester High School
TOTAL OVX GRANTS
Source: http://www.leg.state.vt.us/reports/2008ExternalReports/231758.pdf
IEEE TRANSACTIONS ON INDUSTRIAL INFORMATICS, VOL. 10, NO. 1, FEBRUARY 2014 Architecture for Uniform (Re)Configuration and Processing Over Embedded Sensor and Actuator Networks José Cecilio and Pedro Furtado Abstract—Deployment of embedded systems in industrial the world involve programming every detail of processing and environments requires preconfiguration for operation, and, in
SUTTER MEDICAL FOUNDATION (SMF) 2800 L Street, 7th Floor Sacramento, CA 95816 SMF PCP Treatment & Referral Guideline for Type 2 Diabetes Mellitus Developed July 26, 2006 Revised September, 2011 Diabetes Type 2 .Page 1 Type 2 Diabetes Adult Outpatient Insulin Guidelines………………Page 2 Type 2 Diabetes: Byetta (Exenatide) Guideline…………………….Page 8







