Microsoft word - 010622_ methoxyflurane pi ver 6 clean (updated dosage admin)
PENTHROX® (methoxyflurane) Inhalation
PRODUCT INFORMATION
NAME OF THE MEDICINE
Methoxyflurane is known chemically as 2, 2 – dichloro-1, 1-difluoroethyl methyl ether. The molecular formula is C3H4Cl2F2O and the molecular weight is 164.97. Structural formula:
CAS registry: 76-38-0
DESCRIPTION
A clear, almost colourless mobile liquid, with a characteristic odour. Soluble 1 in 500 of water; miscible with alcohol, acetone, chloroform, ether and fixed oils. It is soluble in rubber. Store in an airtight containers at a temperature not exceeding 40°C. Protect from light. The flash point in oxygen is 32.8°C. The concentration to reach flash point is usually not achieved under normal circumstances.
Methoxyflurane belongs to the fluorinated hydrocarbon group of volatile anaesthetic
agents. It is a volatile liquid intended for vaporisation and administration by
inhalation using the PENTHROX® Inhaler. At low concentrations the inhaled vapour
is used to provide analgesia in stable, conscious patients. Methoxyflurane has a mildly
pungent odour.
SOME OF THE PHYSICAL CONSTANTS ARE:
Molecular weight
Boiling Point at 760 mm Hg
Partition coefficients at 37°C
Blood/gas (mean range)
Vapour pressure 17.7°C
In oxygen (closed system)
Lower limit of flammability of vapour concentration
Methoxyflurane is stable and does not decompose in contact with soda lime. An antioxidant, Butylated Hydroxy Toluene (0.01% w/w) is added to ensure stability on standing. As polyvinyl chloride plastics are extracted by methoxyflurane, contact should be avoided. Methoxyflurane does not extract polyethylene plastics, polypropylene plastics, fluorinated hydrocarbon plastics or nylon.
The vapour concentration of methoxyflurane is limited by its vapour pressure at room temperature to a maximum of about 3.5% at 23°C. In practice, this concentration is not reached due to the cooling effect of vaporisation. Methoxyflurane is not
PENTHROX® (methoxyflurane) Inhalation
flammable except at vapour concentrations well above those recommended for its use.
Recommended concentrations are non-flammable and non-explosive in air and
oxygen at ordinary room temperature.
PHARMACOLOGY
Methoxyflurane vapour provides analgesia when inhaled at low concentrations. After methoxyflurane administration, drowsiness may occur. During methoxyflurane administration, the cardiac rhythm is usually regular. The myocardium is only minimally sensitised to adrenaline by methoxyflurane. In light planes of anaesthesia some decrease in blood pressure may occur. This may be accompanied by bradycardia. The hypotension noted is accompanied by reduced cardiac contractile force and reduced cardiac output.
Biotransformation of methoxyflurane occurs in man. As much as 50-70% of the absorbed dose is metabolised to free fluoride, oxalic acid, difluoromethoxyacetic acid, and dichloroacetic acid. Both the free fluoride and the oxalic acid can cause renal damage in large doses, however dose-related nephrotoxicity seen with clinical doses appears related to a combination of free fluoride and dichloroacetic acid. Methoxyflurane is more susceptible to metabolism than other halogenated methyl ethyl ethers and has greater propensity to diffuse into fatty tissues. Hence methoxyflurane is released slowly from this reservoir and becomes available for biotransformation for many days. Approximately 20% of methoxyflurane uptake is recovered in the exhaled air, while urinary excretion of organic fluorine, fluoride and oxalic acid accounts for about 30% of the methoxyflurane uptake. Studies have shown that higher peak blood fluoride levels are obtained earlier in obese than in non-obese and in the elderly.
INDICATIONS
1. For emergency relief of pain by self administration in conscious haemodynamically stable patients with trauma and associated pain, under supervision of personnel trained in its use (see Dosage and Administration)
2. For the relief of pain in monitored conscious patients who require analgesia for
surgical procedures such as the change of dressings (See Dosage and Administration)
Note: the total maximum dose must not be exceeded.
CONTRAINDICATIONS
• Use as an anaesthetic agent
• Renal impairment, including reduced glomerular filtration rate (GFR), urine
output and reduced renal blood flow.
• Renal failure
• Hypersensitivity to fluorinated anaesthetics
• Cardiovascular instability
• Respiratory depression
• Head injury or loss of consciousness
PENTHROX® (methoxyflurane) Inhalation
• A history of possible adverse reactions in either patient or relatives
• Malignant hyperthermia: patients with known or genetically susceptible to
malignant hyperthermia
PRECAUTIONS
Methoxyflurane impairs renal function in a dose-related manner due to the effect of the released fluoride on the distal tubule and may cause polyuric or oliguric renal failure, oxaluria being the prominent feature. Nephrotoxicity is greater with methoxyflurane than with other halogenated anaesthetics because of the slower metabolism over several days resulting in prolonged production of fluoride ions and metabolism to other potentially nephrotoxic substances. There have also been occasional reports of hepatic dysfunction, jaundice, and fatal hepatic necrosis.
(i) Because of the potential nephrotoxic effects methoxyflurane must not be used
as an anaesthetic agent. The risk is related to the total dose (time and
concentration) and frequent exposure. Methoxyflurane impairs renal function in a
dose-related manner.
Nephrotoxicity is greater with methoxyflurane than with other halogenated
anaesthetics because of the slower metabolism over several days resulting in
prolonged production of fluoride ions and metabolism into other potentially
nephrotoxic substances. Therefore the lowest effective dose of methoxyflurane
should be administered, especially in aged or obese patients.
(ii)
Liver disease: it is advisable not to administer methoxyflurane to patients who
have shown signs of liver damage, especially after previous methoxyflurane or halothane anaesthesia.
(iii)
Diabetic patients: may have an increased likelihood of developing nephropathy if
they have impaired renal function or polyuria, are obese, or are not optimally controlled.
(iv) Daily use of methoxyflurane is not recommended because of nephrotoxic
(v) In patients under treatment with
enzyme inducing drugs (e.g. barbiturates) the
metabolism of methoxyflurane may be enhanced resulting in increased risk of nephrotoxicity.
(vi) Intravenous adrenaline or nor-adrenaline should be employed cautiously during
methoxyflurane administration.
(vii)
Caution in hot climates: Do not expose to temperatures above 40°C, especially
when used in conjunction with oxygen.
PENTHROX® (methoxyflurane) Inhalation
(viii)
Use in the elderly: Caution should be exercised in the elderly due to possible
reduction in blood pressure or heart rate.
(ix)
Health workers who are regularly exposed to patients using PENTHROX®
inhalers should be aware of any relevant occupational health and safety guidelines for the use of inhalational agents. The use of methods to reduce occupational exposure to methoxyflurane, including the attachment of the Penthrox Activated Carbon (AC) Chamber, should be considered. Multiple use creates additional risk. Elevation of liver enzymes, blood urea nitrogen and serum uric acid have been reported in exposed maternity ward staff.
INFORMATION FOR PATIENTS
The decision as to when patients may again engage in activities requiring complete
mental alertness, operate hazardous machinery or drive a motor vehicle must be
individualised. Patients should be warned to take extra care as a pedestrian and not to
drive a vehicle or operate a machine until the patient has completely recovered from
the effects of the drug, such as drowsiness. The treating doctor should decide when
activities such as driving a vehicle or operating a machine may be resumed
. USE IN PREGNANCY
All general anaesthetics' cross the placenta and carry the potential to produce central nervous system and respiratory depression in the new born infant. In routine practice this dose does not appear to be a problem; however in a compromised foetus, careful consideration should be given to this potential depression, and to the selection of anaesthetic drugs, doses and techniques. Neonates delivered of mothers who used methoxyflurane analgesia for childbirth had a briefly raised serum uric acid, not requiring further intervention.
Toxaemia of pregnancy: It is advisable not to administer methoxyflurane due to the
possibility of existing renal impairment.
USE IN LACTATION
Caution should be exercised when methoxyflurane is administered to a nursing
mother.
USE IN CHILDREN
Limited data is available regarding the administration of Methoxyflurane using the
PENTHROX® Inhaler. The minimum effective dose to produce analgesia should be
administered to children.
INTERACTIONS WITH OTHER DRUGS
The concurrent use of tetracycline and methoxyflurane for anaesthesia has been reported to result in fatal renal toxicity. The possibility exists that methoxyflurane may enhance the adverse renal effects of other drugs including certain antibiotics of
PENTHROX® (methoxyflurane) Inhalation
known nephrotoxic potential such as gentamicin, kanamycin, colistin, polymyxin b,
cephaloridine and amphotericin b. Dosage for the subsequent administration of
narcotics may be reduced.
Interactions may occur with β-blockers, with an increased risk of hypotension.
ADVERSE REACTIONS
Note: Use in anaesthesia is contraindicated. No systemic data have been collected on
the frequency or nature of adverse drug reactions of methoxyflurane when used as an
analgesic. There are no data on the dose-dependency of the adverse drug reactions,
therefore all documented adverse reactions are possible, however no statement
regarding frequency can be made.
When used as an anaesthetic:
Common: retrograde
drowsiness, sleeping, dizziness, dislike of odour, fever, polyuria, headache.
non-specific hepatitis, malignant hyperthermia
iii) Other reported events: cardiac arrest, respiratory depression,
laryngospasm, bronchospasm, hypotension, bradycardia, renal failure, increased serum urea, increased serum creatinine, increased urinary oxalate excretion, increased serum inorganic fluoride, pallor, muscle relaxation
Reported in the literature in association with analgesia:
- Nervous system disorders: euphoria, drowsiness, sleepy, agitation,
restlessness, headache, dizziness, dissociation, amnesia
- Respiratory system: cough, choking
- Cardiac hypotension
- Gastrointestinal: nausea, vomiting
- Hepatic: hepatitis, increased liver enzymes
- Renal: increased serum uric acid, urea nitrogen and creatinine
- Eyes: blurred vision, diplopia, nystagmus
Hepatic toxicity in association with methoxyflurane is rare but has been observed with analgesic use.
DOSAGE AND ADMINISTRATION
ANALGESIC
Dosage: Up to 6 mL (2 x 3mL bottles) of PENTHROX® (methoxyflurane) per day,
vaporised in a PENTHROX® Inhaler. If refilling the Inhaler with a second bottle of


PENTHROX® (methoxyflurane) Inhalation
Methoxyflurane, this should occur only once and must be conducted in a well-
ventilated area to reduce environmental exposure to Methoxyflurane vapour.
To maximise safety, the lowest effective dosage of PENTHROX® (methoxyflurane)
to provide analgesia should be used, particularly for children and the elderly. The total
weekly dose should not exceed 15 mL. Administration of consecutive days is not
recommended.
The cumulative dose received by patients receiving intermittent doses of
PENTHROX® (methoxyflurane) for painful procedures (such as wound dressings)
must be carefully monitored to ensure that the recommended dose of methoxyflurane
is not exceeded.
Methoxyflurane may cause renal failure if the recommended dose is exceeded.
Methoxyflurane-associated renal failure is generally irreversible.
PENTHROX® (methoxyflurane) is self-administered under observation (and assisted
if necessary) by a person trained in its administration using the hand held
PENTHROX® Inhaler.
Instructions on the preparation of the PENTHROX® Inhaler and correct
administration are provided in Figure 1.
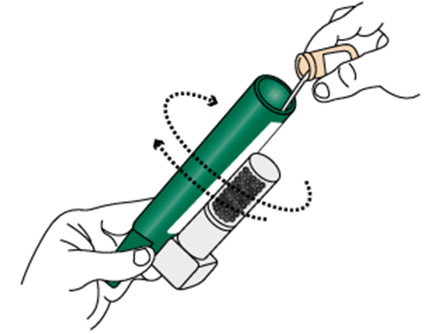
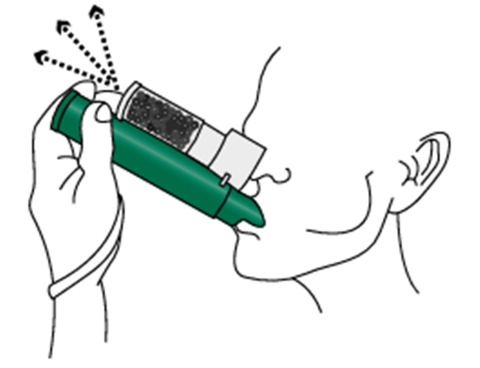
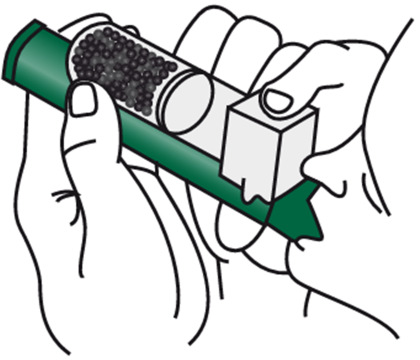
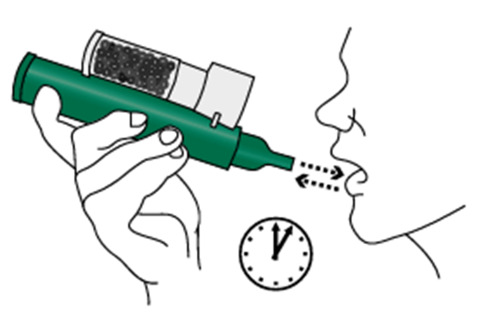
Figure 1 How to use the PENTHROX® Inhaler
Ensure the Activated Carbon (AC) Chamber
1 (where applicable) is inserted into the dilution
hole on the top of the PENTHROX® Inhaler
Holding the methoxyflurane bottle upright, use the base the PENTHROX® Inhaler to loosen the cap
with a ½ turn. Separate the Inhaler from the bottle and remove the cap by hand.
Tilt the PENTHROX® Inhaler to a 45° angle and
3 pour the contents of one 3mL bottle into the base

PENTHROX® (methoxyflurane) Inhalation
Place wrist loop over patient's wrist. Patient inhales through the mouthpiece of Inhaler to
4 obtain analgesia. The patients first few breaths
should be gentle and then breathe normally through Inhaler.
Patient exhales into Inhaler. The exhaled vapour
5 passes through the AC Chamber to absorb any
exhaled methoxyflurane.
If stronger analgesia is required, patient can cover
6 dilution hole with finger during inhalation
Patient should be instructed to inhale intermittently to achieve adequate analgesia.
7 Continuous administration will reduce time of
analgesia. Patients should be administered minimum dose.
OVERDOSAGE
Adverse effects will include those for anaesthetic doses, see Adverse Reactions.
Patients should be observed for signs of drowsiness, pallor and muscle relaxation following methoxyflurane administration.
In the event of excessive urinary output following overdosage, fluid and electrolyte losses should be promptly replaced.
PENTHROX® (methoxyflurane) Inhalation
PRESENTATION & STORAGE CONDITIONS
PENTHROX® (methoxyflurane) is supplied in the following presentations:
a) 3 mL sealed bottle with a tear off tamper seal (pack of 10),
b) Combination pack with one 3 mL sealed bottle and one PENTHROX®
Inhaler (pack of 1 or 10) with or without optional Activated Carbon (AC) Chamber and,
c) Combination pack with two 3 mL sealed bottles and one PENTHROX®
Inhaler (pack of 10).
Store below 30°C
POISON SCHEDULE
NAME AND ADDRESS OF THE AUSTRALIAN SPONSOR
Medical Developments International Pty. Ltd.
A.C.N. 106 340 667
Factory 7, 56 Smith Road
Springvale, Victoria 3171 Australia
Tel: 61-3-9547 1888 Fax: 61-3-9547 0262
NAME AND ADDRESS OF AUSTRALIAN DISTRIBUTOR
2 – 4 Lyonpark Road
North Ryde NSW 2113
Tel: 1800 675 957
Note: Distribution of presentations a) and b) only – refer to Presentation and Storage Conditions section
PENTHROX® (methoxyflurane) Inhalation
NAME AND ADDRESS OF THE NEW ZEALAND SPONSOR
New Zealand Medical and Scientific Ltd.
2A Fisher Crescent
Tel: 64-9 259 4062 Fax 64-9-259 4067
TGA APPROVAL DATE: 13th April 2011
PENTHROX® (methoxyflurane) Inhalation
REVISION HISTORY
Version No.
Amendments
Initials
Update Presentations section. Minor Formatting
changes; Introduction of Marketed version
Update following request from TGA
Update to include Nycomed address and phone number
Presentations section
Update to Dosage and Administration Section to
capture instructions for the use of new base cap
Source: http://www.megamedical.com.au/_literature_115956/Penthrox_Product_Information
Grey in Grey, Noys ‘Grey in Grey': Crisis, Critique, Change This essay reflects on the global financial crisis of 2008 as a site from which to assess a number of theorisations of critique and change, based within a broadly-defined Marxism. While the recent crisis has given traction to Marxism as a form of critique, the articulation of that critique to actual change, and especial y to the prospective agents of change, has been left hanging. Charting the work of Fredric Jameson, Hardt and Negri, and others, we find an emphasis on the powers of production and life as a point of excess to fuel anti-capitalist politics. However, these images of dynamism are now forced to confront capitalism in a state of inertia and deceleration, and in so doing, they reveal their dependence on replicating or displacing the supposed ‘productive forces' of capitalism to their own projects. Models of ‘anti-production', such as those derived from Georges Batail e, also tend to converge on models of vital powers, although cast in forms of consumption and excess. Criticising this convergence on a mythical vitalism, this essay suggests a deflationary critique of capitalism's ‘productivism', and explores the potential for an anti-vitalist analysis that might better grasp the ‘mythological displacement' of experience that operates within the frame of capitalist social relations.
/ APPLICATION NOTE Monitoring Water Vapor in the Lithium-ion Battery Manufacturing Process The lithium-ion battery manufacturing process is sensitive to moisture. This challenging production environment demands a water vapor detection instrument with reliable performance and strong resistance to process byproducts that may be present in the atmosphere. Dry-air management is essential







