Slide

Update on cVEMP and oVEMP
testing in Superior Canal Dehiscence
Erin Piker, AuD PhD
Doug Garrison, AuD

• VEMP Background • Recording a VEMP • Clinical Utility of VEMP • Superior Canal Dehiscence • Case Studies

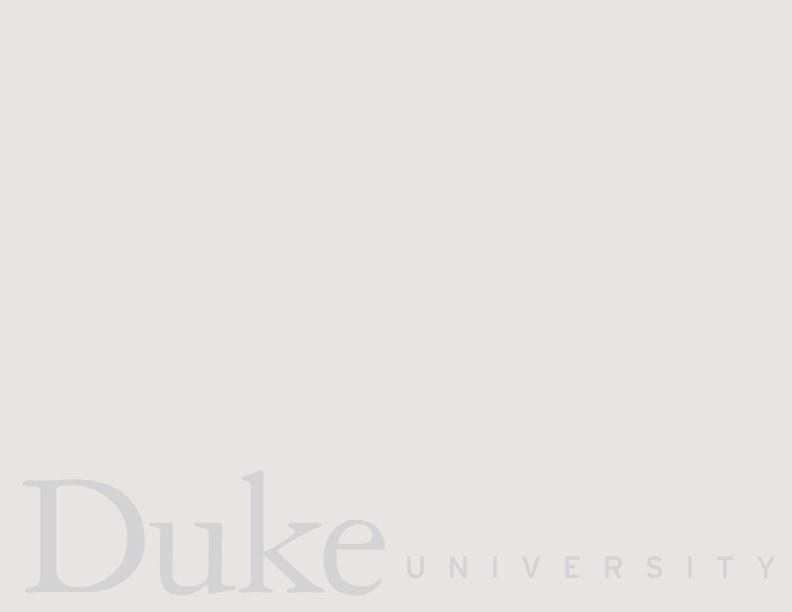
Peripheral Vestibular System
• 3 semicircular canals (SCC)
– Angular acceleration and deceleration
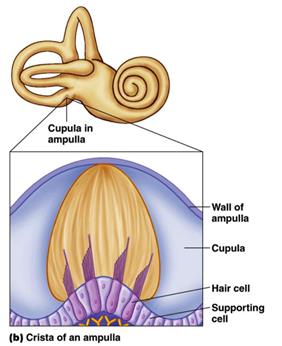
• Utricle and saccule
– Linear acceleration and deceleration

Vestibular Evoked Myogenic Potentials
• In addition to movement, vestibular afferents may be activated
– Sounds of high intensity – vibration and – electrical stimulation applied over the mastoid process
• Then a series of reflexes are triggered that include short latency
activations and inhibitions of electromyographic (EMG) activity
• EMG: measures the modulation of muscle activity • When mediated through the vestibular end organs referred
to as vestibular evoked myogenic potentials (VEMP)
• We are using sound only
as a pressure stimulus
• i.e. sound pressure is
being used as a hydro-
mechanical force to move
the endolymphatic fluid
and, as a consequence, to
translate otoliths to
create transduction
Slide courtesy of Gary Jacobson
Vestibular Evoked Myogenic Potentials
• A VEMP recorded from the
• A VEMP recorded from the
SCM = cervical VEMP
EOM = ocular VEMP
adapted from Curthoys 2010
• Afferent pathway
– Inferior vestibular nerve
• Central connections
– vestibular nucleus
• Efferent pathway
– Medial or lateral
vestibulospinal tract to the
spinal accessory nucleus
of cranial nerve XI
– Cranial nerve XI innervates
the motor neurons of the
adapted from Iwasaki et al, 2008
• Afferent pathway:
– superior vestibular nerve
• Central connections:
– vestibular nucleus
• Efferent pathway
– medial longitudinal
fasciculus (MLF) routes to
cranial nerve III
– CN III innervates four of
the six extraocular muscles
– Contralateral inferior
Recording a VEMP
• Air conduction (e.g. click or tone burst) • Bone conduction (e.g. B-71) • Mechanical taps (tendon/reflex hammer) • Galvanic stimulation • AC tone bursts are most common in use clinically
– AC is feasible and accessible – Low frequency tone burst - large amplitude response
Stimulus Characteristics
(both cVEMP and oVEMP)
Stimulus Type
500 Hz tone burst, 2-0-2 cycle, Blackman gated; 100 usec click
Transducer
ER3a insert earphone
Intensity
Recording Characteristics
Sweeps per average
Artifact Rejection
Patient set-up and Electrode montage
Supine, head turned away from
Supine/sitting, gazing upward
stimulus and lifted
Non-Inverting/Active cVEMP: ipsi SCM oVEMP: contra IO
Inverting/Reference cVEMP: sternum, chin, hand oVEMP: below non-inv.
cVEMP versus oVEMP
• cVEMP waveform is
positive/negative
• oVEMP waveform is
negative/positive
• Peak-to-peak amplitude • Peak latency • Threshold • Interaural amplitude, latency, and threshold
VEMP Parameters: Threshold
• cVEMP, 500 Hz TB
• oVEMP, 500 Hz TB
– 15 – 350 uV
• IAA: > 44%
• IAA: > 33%
– Mean Range: 11.81 –
– Mean Range: 8.77 –
– Cut-off: >20.47
– Cut-off: >14.4
• ILD: >3.39
• ILD: > 2.47
Zapala & Brey 2004; Piker et al. 2011; Li et al. 2014
Subject Variables that can affect the VEMP
• Conductive hearing loss
– Stimulus can't reach the inner ear at an
– Must use bone conduction or taps
Yang & Young (2003) • Patient with right
• Tone-burst VEMP
present in left ear, absent in right
• Tapping produced
VEMPs bilaterally
Subject Variables that can affect the
• Patient's ability to
– cVEMP – Voluntary tonic EMG
influences the cVEMP No EMG
– Linear relationship
between cVEMP amplitude and degree
Akin et al. 2004
of SCM contraction
Subject Variables that can affect the
• Gaze direction (oVEMP)
– oVEMP amplitude is
greatly effected by gaze
Govender, Rosengren, & Colebatch (2009)
Subject Variables that can affect the
– VEMPs can be recorded
across the lifespan, from
neonates to elderly
– Neonates show increased
latencies and smaller
amplitudes (e.g. Chen et al. 2007)
– Older adults show smaller
amplitudes, increased
latencies (maybe?),
increased thresholds, and
reduced response rate (i.e.
not all older adults will
produce a VEMP in response
to air conduction stimulus)
Piker et al. 2012
Clinical Utility of VEMP
Clinical use of VEMPs
Curthoys & Manzari, 2013
Vestibular Neuritis
• Using both cVEMP and oVEMP can localize superior vs
inferior nerve involvement
– oVEMP measuring utricle and superior vestibular nerve – cVEMP measuring saccule and inferior vestibular nerve
• If patient has superior vestibular neuritis, should have
impaired oVEMP on that side but cVEMP should be normal
• If patient has inferior vestibular neuritis, patient should
have preserved oVEMPs bilaterally and the cVEMP should be absent on side of neuritis
Example of Inferior Vestibular Neuritis
• Prior to our ability to assess the inferior
cVEMP: Abnormal, 50% asymmetry
nerve and localize the impairment, many patients with IVN were mistaken for central vestibular disorders (Kim & Kim, 2012)
Jacobson, McCaslin, & Piker (2011)
Clinical use of VEMPs
• cVEMP and oVEMP also used in evaluation of many
other pathologies when function of the vestibular system is questioned
– e.g. vestibular neuritis, Meniere's Disease, migraine-
associated vertigo, multiple sclerosis, superior canal dehiscence (SCD)
• One of the clinical limitations of VEMP tests is that,
as with most vestibular tests, VEMPs assess site of lesion…not necessarily the presence or absence of disease
Clinical use of VEMPs
• cVEMPs abnormal in cases of IVN, while oVEMPs and caloric testing are usually
– However, the diagnosis of inferior neuritis is ultimately based on case history
• cVEMPs are hypothesized to be useful in Meniere's Disease because the saccule
is believed to be the second most involved structure in endolymphatic hydrops
– However, the sensitivity and specificity of cVEMPs are reportedly only 50% and
48.9%, respectively, in patients with unilateral definite Meniere's Disease
• VEMPs are not essential for the diagnosis of migraine
– but it may be important to quantify vestibular involvement
• Patients with utricle and saccule impairments, as measured using cVEMP and
oVEMP tests, may be more susceptible to BPPV since the otoconia responsible for canalithiasis originate in the otolith end organs
Hong et al., 2011; Kim & Kim, 2012; Egami et al., 2013
Clinical use of VEMPs
• Research still working towards defining the value of the
VEMP in most of these pathologies
– e.g. Should we expect otolith or nerve impairment in this
disease? How sensitive are the tests to such an impairment?
• But….VEMPs have proven to be VERY EFFECTIVE at
measuring the presence of disease in cases of superior canal dehiscence (SCD)
Superior Canal Dehiscence
Superior Canal Dehiscence
• History • Etiology • Pathophysiology • Symptoms • Audiogram • Vestibular Testing • CT Scan • Treatment
Superior Canal Dehiscence
Minor et al, 1998
• 8 cases identified over 2 year period • Chief complaint: vertigo, oscillopsia, dysequilibrium
related to sound, changes in middle ear pressure, changes in intracranial pressure
• 7 of 8 showed vertical/torsional eye movements
induced by sound and/or pressure
• Dehiscence confirmed by CT scan • Two patients underwent surgical plugging
Sound and pressure induced vertigo
• Tullio Phenomenon
– first identified in patients with congenital syphilis – later reported in cases of congenital deafness, perilymph
fistula, head trauma, Lyme Disease and canal erosion
associated with cholesteatoma
• Hennebert Sign
– First associated with congenital syphilis – Later reported in cases of Meniere's Disease due to adhesions
between stapes and membranous labyrinth
• Cawthorne, 1956, postulated these symptoms were due to
disruption of the bony labyrinth causing a third ‘mobile
window' of the vestibule
Superior Canal Dehiscence
• An abnormality of the temporal bone showing an
absence of bone where the roof of the superior semicircular canal meets the floor of the middle cranial fossa
– 5/1000 temporal bones with dehiscence – 14/1000 temporal bones with thinning (<0.1mm) – 1.9% prevalence was thought to be conservative
SCD – How is it Diagnosed
• History and Symptoms • Audiologic and vestibular testing • CT scan
– Near sagittal fine cut CT through the plane of the
– Fine cuts are 0.3 to 0.5mm thickness
• Congenital Malformation
– Half of individuals with thinning or dehiscence were
– Dehiscence visually looked similar to INFANT temporal
• Normal development shows thickening until 4 years of age
• Trauma • Increased Intracranial Pressure
SCD and Spontaneous CSF Leak
• Retrospective chart review of patients undergoing
surgical repair of spontaneous CSF leak
– Excluded for history of trauma, cholesteatoma, neoplasm – 5 of 31, 16%, with spontaneous CSF leak had visually
confirmed dehiscence
• Incidence of CSF leak is greater in patients with
intracranial hypertension as higher pressure causes
erosion of temporal bone
• Cases of spontaneous CSF leak present to audiology
clinics as superior canal dehiscence
SCD and Chiari Malformation
• Prevalence of Chiari Type I: 0.6% – 1.0%
– The cerebellar tonsils are displaced downward into the
foramen magnum and this results in overcrowding of the
posterior cranial fossa
• Retrospectice chart review over 8 years of patient
diagnosed with SCD
– 7 of 30 patients (23%) diagnosed with canal dehiscence
also had radiographically identified Chairi Type I
• Most dehiscence located at posterior canal • Chiari results in obstruction of CSF flow which may
lead to slow erosive process at posterior cranial fossa
Normal Physiology-Air Conduction
• As the stapes pushes INWARD at the oval window,
pressure is exerted upon the perilymph within the
• Because fluids are essentially incompressible AND
the round window offers an outlet via OUTWARD
movement, this pressure wave moves into the
cochlea via the scala vestibuli and out via the scala
• The basilar membrane is conveniently positioned in
the scala media to take advantage of the impedance
inequality between the two windows
Normal Physiology-Air Conduction
Merchant and Rosowski, 2008
Abnormal Physiology-Air Conduction
Merchant and Rosowski, 2008
Abnormal Physiology-Air Conduction
• When a ‘third window' is introduced, the
impedance relationship changes such that the round window is no longer the only outlet.
• The dehiscence permits the fluid pressure to
divert into the vestibular portion of the membranous labyrinth and the result is less fluid pressure moving into the scala vestibuli
• One result is decreased sensitivity to AC stimuli
Normal Physiology-Bone Conduction
• When the temporal bone is vibrated, there is an
impedance inequality between the scala vestibuli and scala tympani.
– Again, this is due to an impedance inequality between
the oval and round windows
• Normal hearing is predicated on appropriate
impedance of the inner ear and across those two windows
Normal Physiology-Bone Conduction
Merchant and Rosowski, 2008
Abnormal Physiology-Bone Conduction
Merchant and Rosowski, 2008
Abnormal Physiology-Bone Conduction
• When the temporal bone is vibrated and those
vibrations are able to escape via a ‘third window', it disrupts the normal impedance relationship between the oval and round windows.
• This occurs by decreasing impedance on the scala
vestibuli side and the result is enhanced movement of the cochlear partition.
• One result is increased sensitivity to BC stimuli
Questions on Pathophysiology?
Vestibular Signs and Symptoms
• First description of this pathology included solely the
vestibular symptoms
– Oscillopsia – Tullio Phenomenon and vertical/torsional nystagmus to
sound or possibly own voice
– Hennebert Sign and vertical/torsional nystagmus to
• Chronic Dysequilibrium • Positional Vertigo • Head tilt in response to sound
Audiologic Signs and Symptoms
• Aural fullness • Autophony
– Own voice echoes, excessively loud
• Amplified body noises
– Pulsatile tinnitus, eye movements, feet striking ground
• Hearing loss
– Low frequency air-bone gaps with normal immittance – ‘Inner ear conductive'
Other "Inner Ear Conductive" Hearing
Loss - Enlarged Vestibular Aqueduct
• Prospective study
– 8 ears from 5 individuals identified in routine clinical practice – CT scan confirmed EVAS
• vestibular aqueduct greater than 1.5 mm on CT scan
• Seven of 8 showed low frequency air-bone gaps • Six of 8 showed normal tympanogram • Acoustic reflexes present in 3 of 4 ears tested • One middle ear surgical exploration normal • Agrees with pathophysiology of third mobile window
proposed by Merchant and Rosowski
– Raises interesting questions about hearing loss type in EVA
Dehiscence Size and Symptoms
• Size of Dehiscence correlated with symptoms • 27 patients identified prospectively
– Dehiscence at least 2.5mm showed cochlear AND
vestibular signs and symptoms
– Dehiscence less than 2.5mm showed either cochlear
OR vestibular signs and symptoms
• Larger the dehiscence, the greater the symptoms
Size of Dehiscence and ABG
• Size of air-bone gap correlated with size of
• Retrospective case review of 23 patients
– Air-bone gap with every dehiscence over 3mm
• Average size of ABG correlated with average size
SCD is great otologic mimicker
• Otosclerosis
– Stapedectomy, ossiculoplasty doesn't help – Likely diagnosed if symptoms center around hearing
• Perilymphatic Fistula
– Packing middle ear doesn't help – Likely diagnosed if symptoms center around dizziness
• Meniere's Disease
– Low salt diet, diuretic doesn't help
• Eustachian Tube Dysfunction
– Nasal Steroids don't help
SCD – Not Otosclerosis
• Eight patients, 10 ears found via retrospective
• All 10 ears had conductive hearing loss • No patient presented with vestibular complaints • 6 individuals had surgical exploration for assumed
• All middle ear surgeries unsuccessful
SCD – Not Otosclerosis
SCD – Not Otosclerosis
SCD – Key Audiometrics
• Air-bone gap
– This may be BC thresholds below zero and AC thresholds
• Normal immittance
– Normal tympanogram – Present acoustic reflexes
• Subjective dizziness with tympanogram, ‘fistula test' • Bone oscillator to ankle localizes to affected ear • VEMPs!!
• Surgical Intervention
• Surgery takes 3 hours • Patient spends 3 nights in hospital • If successful, vestibular dysfunction guaranteed • "repair of SCD reduce the function of the operated canal but typically
preserve function of the other semicircular canals"
• Apparently more difficult, results variable
– Knowledge is Power – Expectations drive satisfaction
Treatment in Literature
3/27 middle fossa approach with canal plugging
– One patient ‘fixed' – Two patients closed ABG, but now unsteady
10/27 middle fossa approach with canal plugging
– Five showed no change in post-op ABG – Two recurrent
18/19 middle fossa approach with canal plugging, 1 resurfaced
– Two showed complete vestibular loss – Six showed various degrees of vestibular dysfunction of other semicircular canals based on head
– Resurface showed dysfunction of posterior canal
10/11 middle fossa approach with canal plugging, 1 resurfaced
– Four showed high frequency hearing loss – Two showed non-operated ear symptomatic – Two showed transient BPPV – Resurfaced showed no improvement
Possible Complications from Treatment
• Prolonged Hospital Stay • Possible Hearing loss
– Persistent low frequency conductive – High frequency sensorineural – Profound sensorineural
• Possible Vestibular Dysfunction
– Plugged canal non-functioning – Horizontal or posterior canal deficit – BPPV
• If bilateral, non-operated side becomes symptomatic
• VEMP tests can be used to detect whether a
dehiscence is causing pathological pressure
transmission in the vestibular labyrinth
• In healthy ear, sound stimuli activate the otolith
organs leading to inhibition of SCM and excitation of
extraocular muscles cVEMP and oVEMP
• In SCD, the dehiscence acts as a "third mobile
window" – effectively creating a path of lower
impedance for the transmission of sound pressure to
• VEMPs are larger in amplitude • Threshold to elicit VEMP is reduced
Old Criteria: cVEMP Threshold
• cVEMP amplitudes tend to be larger in SCD
ears….but the intra-ear variability in cVEMP
amplitude precludes it from separating SCD ears
from healthy ears
– In other words, there is a great deal of overlap in
cVEMP amplitude between healthy individuals and
– Sensitivity 74%
• cVEMP parameter of most interest for the
identification of SCD has been the cVEMP
Janky et al. 2014
• Average cVEMP threshold using an air conduction
tone burst of 500 Hz in a normal ear is around 85 -
• Average cVEMP threshold in an SCD ear is between
Watson et al. 2000; Streubel et al. 2001; Zhou et al. 2007; Brandtberg et al. 2009;
– Sensitivity ranges from 80 – 91%, specificity 80 – 95% – Non-invasive
• Disadvantages
– Takes time and multiple test runs – Patient can fatigue – Variable cut-offs
• i.e. definition of "normal" and "pathological" threshold
differ by site and study
cVEMP Threshold
Sensitivity
Specificity
• 20 dB nHL range between recommended cut-off values???
Zhou et al. 2007; Crane et al. 2008; Zuniga et al. 2013
New Criteria: oVEMP Amplitude
• oVEMP thresholds tend to be 10 dB nHL
lower in SCD patients….but oVEMP amplitudes are often ten times larger in an SCD ear!
• Mean amplitudes:
• Normal = 2.9 uV (3.0) • SCD = 29.0 uV (16.6)
Janky et al. 2014
• 29 patients with surgically confirmed SCD, 25 age-matched
• Looked at whether oVEMP amplitudes were more sensitive
and specific than cVEMP thresholds for the diagnosis of SCD
Zuniga et al. (2013)
• Mean SCD cVEMP threshold = 75 dB nHL • Mean Control cVEMP threshold = 95 dB nHL
Zuniga et al. (2013)
Zuniga et al. (2013)
• Mean SCD amplitude = 48.9 uV • Mean Control amplitude = 3.8 uV
Zuniga et al. (2013)
Zuniga et al. (2013)
oVEMP amplitude: best cut-off differs by age, sensitivity 90 – 100% and specificity 94 – 100%
cVEMP threshold: best cut-off differs by age, sensitivity 45 – 100% and specificity 46 – 100%
Other single-step oVEMP tests?
• 22 CT-verified SCD subjects, 22 healthy controls • Purpose was to find a single-step screener that
separated SCD from healthy ears
• Ran oVEMPs at multiple frequencies • 100% of SCD subjects generated oVEMPs at 4000 Hz,
no healthy controls did
oVEMP, 4000 Hz, 95dBnHL
• 500 Hz oVEMP: Left = 71.2 uV, Right = 6.69 uV • 4000 Hz oVEMP: Left = 37.33 uV, Right = absent
4.98 ms/div, 10 uV/div
4.98 ms/div, 10 uV/div
Thank you, Gary Jacobson
• Clinical gold-standard is still a CT scan • But VEMP testing plays a key role in determining
whether the apparent dehiscence is actually causing pathologic pressure transmission in the inner ear
• Why is that important?
CT scan of pt with complete dehiscence in left ear
CT scan of pt WITH0UT complete dehiscence
• "CT imaging alone can be misleading in the diagnosis of SCD. It can overestimate the
size of the dehiscence, and can falsely detect dehiscences."
• "CT cannot be used in isolation for the diagnosis of SCD."
• Clinical symptoms and signs and test results must
be clearly indicative before definitive diagnosis, and definitely before surgery
• Diagnosis needs to be based on combination of
patient symptoms, CT findings, and VEMPs
• 66 y/o female • Reports constant disequilibrium for 13 years, getting worse • "She reports Tullio Phenomenon, dizziness with cough, sneeze,
strain, exertion, bending. She also reports left autophony, aural
fullness, left pulsatile tinnitus that is essentially constant"
• Reports a previous vestibular work-up at outside facility that
showed normal VNG
• Audio from 2000 showed a mild conductive hearing loss in left
• 2001 exploratory left ear surgery looking for a fistula (none was
CASE 1: Vestibular Testing
• VNG exam: normal • Rotary chair exam: normal • VEMP: "Cervical and ocular VEMPs are present
on the left, absent on the right. Ocular VEMP shows absolute amplitude of 24uV which is abnormal. Subthreshold cVEMPs are absent. Presence of any VEMP measure on the left, given large ABG in the left, is abnormal and indicates superior canal dehiscence."
Case 1: Vestibular Testing
• Left oVEMP amplitude = 24 uV • Right oVEMP absent
Case 1: Vestibular Testing
• Left cVEMP present at 90dBnHL despite 60 dB
• Right cVEMP absent
CASE 1: Treatment
• CT scan confirmed left SCD • Patient decided to proceed with a left middle
fossa craniotomy to repair the dehiscence via canal plugging
CASE 1: Post-Op Audio
• Patient reports
sudden hearing loss
one day after surgery
• Pulsatile tinnitus has
• Autophony resolved • Imbalance improved
initially, able to drive
• 1 month later stated
she felt persistent
CASE 1: Follow-up
• Underwent PT for balance • Referred for single sided deafness workup to
discuss options (e.g. CROS vs BAHA)
– Opted to get a BiCros hearing aid
Case 1: Discussion
• History of previous middle ear surgery looking for a cause
of symptoms and ABG
– No cause found, probably resulted in ME CHL
• Audio shows 65 dB ABG, some of it ME CHL, some of it
enhanced BC due to SCD
– Normal tymps, reflexes not completed
• Present VEMPs with large ABG • "Classic" SCD symptoms, very bothersome, chose surgical
• Outcome of surgery was poor (total loss of hearing in left
ear, chronic imbalance)
• 53 y.o. male • Complains of chronic dizziness for 10 years, began after
• Increase in tinnitus • Double vision • Surgical procedure to repair perilymphatic fistula,
• No help with vestibular rehabilitation therapy • Patient reports prior CT ruled out SCD • Medical history significant for variety of other health
• "Mild conductive hearing loss in both ears in the low
• Normal tympanograms, bilaterally • Acoustic reflexes not performed • Second CT scan showed ‘rather large' dehiscence of
right superior canal involving entire dome of the canal and probable thinning of left superior canal
• Spinal tap showed increased CSF pressure
Case 2: Vestibular Testing
• Right cervical VEMP threshold = 65dBnHL • Left cervical VEMP 70dB screening negative
Case 2: Vestibular Testing
• Ocular VEMP amplitude = 22.5 uV
Case 2: Follow-up
• Air-bone gap closed • Cervical VEMP threshold increased • Still some dysequilibrium at 9 months post-op • Spinal tap showed increased intracranial pressure
– CSF drainage offered no relief
• Dysequilibrium improving at one year with VRT,
but still present
Case 2: Follow-up Testing
threshold 95dBnHL
• No change on
Case 2: Discussion
• History of previous middle ear surgery looking for a
• "Classic" SCD symptoms and history of previous
work-up for SCD, negative
• cVEMP threshold and oVEMP amplitude consistent
with SCD in right ear
• Chose surgical plugging • Outcome of surgery was good • cVEMP threshold back to WNL post-surgery
• 61 y/o female • January 2013
– c/o of right pulsatile tinnitus and right aural fullness – NO VESTIBULAR COMPLAINTS – Audio:
• "mild to moderate CHL right ear, NL hearing left ear". • Tympanometry: Type C tymps bilaterally (-148 R, -144 L)
– Diagnosed with right Eustachian Tube Dysfunction – Treated with Flonase, f/u in month
• February 2013
– Same complaints, no change in symptoms – PE tube placed in right TM
– Still c/o of right tinnitus and fullness, now complains
of right hearing loss
– Prior to f/u had seen neurosurgery to follow-up on
previous history of right cerebral AVM, neuro ordered CT
– CT showed possible SCD in right ear – She is referred for vestibular testing
Case 3: Vestibular Testing
• VNG: not completed due to PE tube
Case 3: Vestibular Testing
– Left ear = absent – Right ear = 276.95
uV at 100 dB nHL and threshold at 85 dB nHL
Case 3: Vestibular Testing
– Left ear = absent – Right ear = 25.78
uV at 100 dB nHL
Case 3: Vestibular Testing
• "Results consistent with right SCD (i.e. any VEMP
response in the presence of a 45 dB ABG is significant. Larger ocular VEMP response on the right provides further evidence of this. Absent response on left may be due to significant negative middle ear pressure."
Case 3: Follow-up
• Elected not to have surgery as her symptoms do
not bother her very much and she has no vestibular symptoms
Case 3: Discussion
• Presumed to have ETD (fullness and CHL in ear) • No vestibular symptoms • History of PE tube due to ETD
– not sure if ETD was truly present, but procedure did not
resolve symptoms and resulted in ME CHL
• SCD incidental finding on CT looking for evidence of
• cVEMP threshold and oVEMP amplitude consistent
with SCD – especially given the 45 dB ABG, some of
which was most likely ME conductive
• 58 female • Complained of:
– spinning vertigo, lasting seconds, that occurred when
– chronic disequilibrium – constant pressure in right ear that increased when
• Had been evaluated by multiple ENTs over several
years, told nothing wrong with her ear
Case 4: Audiogram
Case 4: Vestibular Testing
• VNG: Normal • Rotational Testing: Normal • cVEMP: Normal • oVEMP Abnormal
• Present and symmetrical • Screened at 75 dB nHL, response absent
• Absent in left ear (patient age?) • Right ear amplitude = 93 uV
Case 4: Temporal Bone CT
The radiologist reported a "bony dehiscent of the superior semicircular canal bilaterally"
Case 4: Follow-up
• Though the CT scan identified bilateral SCD, based
on symptoms and oVEMP results the patient was ultimately diagnosed with SCD in the right ear only
• During follow-up with our otolaryngology
colleague, she decided not to undergo surgical treatment….but expressed gratitude and relief in finally having a diagnosis and no longer feeling like she was "going crazy"
Case 4: Discussion
• The patient's symptoms did not include all the "classic" SCD
symptoms that typically trigger the suspicion of SCD (i.e. she denied
autophony or dizziness in response to loud sounds)
– Her main complaint was aural fullness in the right ear
• Based solely on her symptoms and normal cVEMP thresholds, a
diagnosis of SCD would most likely not have been reached
– would she have continued to search for an answer to her symptoms?
• She may have a low frequency CHL
– Though BC on audio not completed – should it be if hearing is normal
but patient complains of fullness or other SCD-like symptoms?
• Relying solely on her CT report may have resulted in a diagnosis of
– may have caused an increase in health anxiety for the patient given
her lack of symptoms on the left side
• oVEMP amplitude is what raised suspicion of SCD, and combination
of oVEMP and symptoms led to diagnosis of right-sided SCD only
(even though CT scan interpreted as showing a bilateral dehiscence)
• Cervical VEMP-saccule and inferior vestibular nerve • Ocular VEMP-utricle and superior vestibular nerve • VEMPs are sensitive and specific to SCD because
provide an objective measure of abnormal pressure
transmission in inner ear
– cVEMP threshold decreases – oVEMP response amplitude increases (may be more
sensitive than cVEMP threshold)
– oVEMP response is recordable up to 4kHz
• CT scan at risk for overdiagnosing SCD - difficulty
differentiating between ‘thinning' and true dehiscence
– and results need to be corroborated with symptoms
• Audiogram will likely show
– Air-bone gap with normal immittance – May see BC thresholds below 0
• SCD complaints may be cochlear, vestibular or both • Surgical treatments for SCD have the potential to
improve some symptoms, possibly not all.
• Surgical treatment may lead to other balance
problems and/or hearing loss
• Questions/comments?
Source: http://www.ncshla.org/sites/default/files/fallCon/2014/Session-27.pdf
GOVT. OF MAHARASHTRA OFF SITE DISASTER MANAGEMENT PLAN FOR JALNA DISTRICT Office of Joint Director, Industrial Safety & Health, Aurangabad. In the recent past, we have experienced Industrial Disasters of serious nature. One of which is Bopal tragedy, one cannot forget. The outcome of such disasters resulted in tremendous increase in awareness of people all over the world. Governments of various countries world-wide have taken prompt action in preventing such Disasters & formalising mitigation activities in case of eventualities. Various groups, institutions, authorities are constantly working / updating such action plans. Under the leadership of District Collector Mr. Shyam Deshpnade & Technical guidance of Mr. B.N.Kalaskar Jt. Director DISH, this Disaster Control plan is prepared. The objective of this plan is to increase awareness of Industry Management in view of mitigating the eventualities & to provide them necessary information with regard to resources available in the District. This plan deals with Industrial Disasters only. One MAH unit is identified by DISH office & list of other chemical handling factories has been given herewith. In the year 1989, Central Govt. enforced the rules "Environment Protection Act" known as Manufacture, Storage & Import of Hazardous Chemicals Rules 1989. Under the said rules statutory provisions were laid down for preparation of On-site Emergency Management Plan by the occupiers of the Major Accident Hazard factories & Off-site Disaster Control Plan by the District Collector / District Emergency Authority designated by State Govt. The Central Govt. subsequently Gazzeted additional rules in August 1996 making additional provisions with regard to Emergency Planning Preparedness & Response for chemical accidents. These rules are known as "Chemical Accidents" (Emergency Planning, Preparedness & Response) Rules 1996. Under these rules Central / State / District / Local crises groups are required to be constituted. The District crises group has to assist in the preparation of the District Off- Site Disaster Control Plan. This off-site Disaster Control Plan is prepared taking into consideration aforesaid legal requirement.
VOLUME 16, NUMBER 1 August 2009 AN IEER PUBLICATION Radioactive Rivers and Rain: Routine Releases of Tritiated Water From nuclear Power PlantsBy annIe MakhIjanI and arjun MakhIjanI, ph.d.nuclear power plants generate tritium in the course of their operation and release it both to the atmosphere and to water bodies. tritium







