Effect of reiki therapy on pain and anxiety in adults: an in-depth literature review of randomized trials with effect size calculations
Effect of Reiki Therapyon Pain and Anxiety inAdults: An In-DepthLiterature Review ofRandomized Trials withEffect Size Calculations
- - - Susan Thrane, RN, MSN, OCN,
and Susan M. Cohen, PhD, APRN, FAAN
- ABSTRACT:The objective of this study was to calculate the effect of Reiki therapyfor pain and anxiety in randomized clinical trials. A systematic searchof PubMed, ProQuest, Cochrane, PsychInfo, CINAHL, Web of Science,Global Health, and Medline databases was conducted using the searchterms pain, anxiety, and Reiki. The Center for Reiki Research also wasexamined for articles. Studies that used randomization and a controlor usual care group, used Reiki therapy in one arm of the study, werepublished in 2000 or later in peer-reviewed journals in English, andmeasured pain or anxiety were included. After removing duplicates,49 articles were examined and 12 articles received full review. Sevenstudies met the inclusion criteria: four articles studied cancer patients,
From the University of PittsburghSchool of Nursing, Research in Cancer
one examined post-surgical patients, and two analyzed community
dwelling older adults. Effect sizes were calculated for all studies using
Cohen's d statistic. Effect sizes for within group differences rangedfrom d ¼ 0.24 for decrease in anxiety in women undergoing breast
Address correspondence to SusanThrane, RN, MSN, OCN, University of
biopsy to d ¼ 2.08 for decreased pain in community dwelling adults.
Pittsburgh School of Nursing, 3500
The between group differences ranged from d ¼ 0.32 for decrease of
Victoria Street, Victoria Building,
pain in a Reiki versus rest intervention for cancer patients to d ¼ 4.5
Pittsburgh, PA 15261. E-mail:
for decrease in pain in community dwelling adults. Although thenumber of studies is limited, based on the size Cohen's d statistics
Received April 6, 2013;
calculated in this review, there is evidence to suggest that Reiki ther-
Revised July 12, 2013;Accepted July 12, 2013.
apy may be effective for pain and anxiety. Continued research usingReiki therapy with larger sample sizes, consistently randomized
This study was supported by NINR
groups, and standardized treatment protocols is recommended.
Ó 2013 by the American Society for Pain Management Nursing
1524-9042/$36.00Ó 2013 by the American Society for
The use of complementary and alternative medicine (CAM) techniques is grow-
Pain Management Nursing
ing in popularity with the public. CAM modalities are often either lauded or de-
bunked in the popular press and the scientific community based on the evidence
Pain Management Nursing, Vol -, No - (--), 2013: pp 1-12
of one study. Reiki therapy, a form of biofield energy,
of hand positions. Most people leave a Reiki therapy
has been examined in community dwelling older
session feeling very relaxed. A qualitative study found
adults, in specific disease conditions such as cancer,
that during a Reiki treatment participants felt ‘‘dreamy,'
chronic fatigue, diabetic neuropathy, in surgical pa-
‘‘safe,' ‘‘secure,' and ‘‘more grounded'' (p.
tients, and in other patient populations. The objective
255). A study of nurses who use Reiki therapy for
of this review is to determine if Reiki therapy is effec-
self-care found that the nurses used Reiki therapy dur-
tive for pain and anxiety in adults and to calculate the
ing their workday to feel more calm, centered, and
effect sizes for Reiki therapy in randomized clinical tri-
more able to care for others (
als. Moreover, this review considers the use of Reiki
The National Center for Complementary and Al-
therapy for pain and anxiety in adults and seeks to dis-
ternative Medicine (NCCAM) places Reiki therapy in
cover if Reiki therapy is effective for these conditions
the category of biofield energy. Biofield energy is any
based on current evidence.
electrical or magnetic field produced by a biological or-
There is a lot of confusion about what Reiki ther-
ganism, e.g., a human. The human body produces mea-
apy is. From a practical standpoint, Reiki therapy is
surable electrical and magnetic fields. The heart
a way for the practitioner to guide energy to the recip-
produces an electrical field to regulate its beat. This
ient, to assist the innate healing energy of the recipient,
electrical signal is measured through an electrocardio-
and to facilitate self-healing (
gram (ECG or EKG), a common medical test. The brain
also produces an electrical field but at a much lower
The practitioner does not cause the healing, nor are
level than the heart. In fact, every cell in the human
they the source of the energy. The practitioner is
body produces minute amounts of electricity, a mag-
a channel for the energy, much like a garden hose is
netic field, has a positive charge on the outer cell
a channel for water. Many call this energy universal,
wall, and has a negative charge on the inner cell wall
but some say it is from God, Buddha, or a sacred
(). Electrical fields produce magnetic fields,
source. A common interpretation of the word Reiki is
with a stronger electrical field producing a stronger
spiritually guided life force energy ().
There are several versions regarding the origins of
magnetic resonance imaging (MRI) scan uses the
Reiki therapy. It is generally accepted that Reiki ther-
body's own magnetic field (along with a strong
apy began with Dr. Mikau Usui, a spiritual seeker
magnet and radio waves that are emitted from the
who undertook a 21-day penance and fast on Mount
machine) to produce sharp images of soft tissue
Kurama in Japan ). Usui experienced the
within the body (Classic Newtonian
Reiki energy on the twenty-first day and was healed.
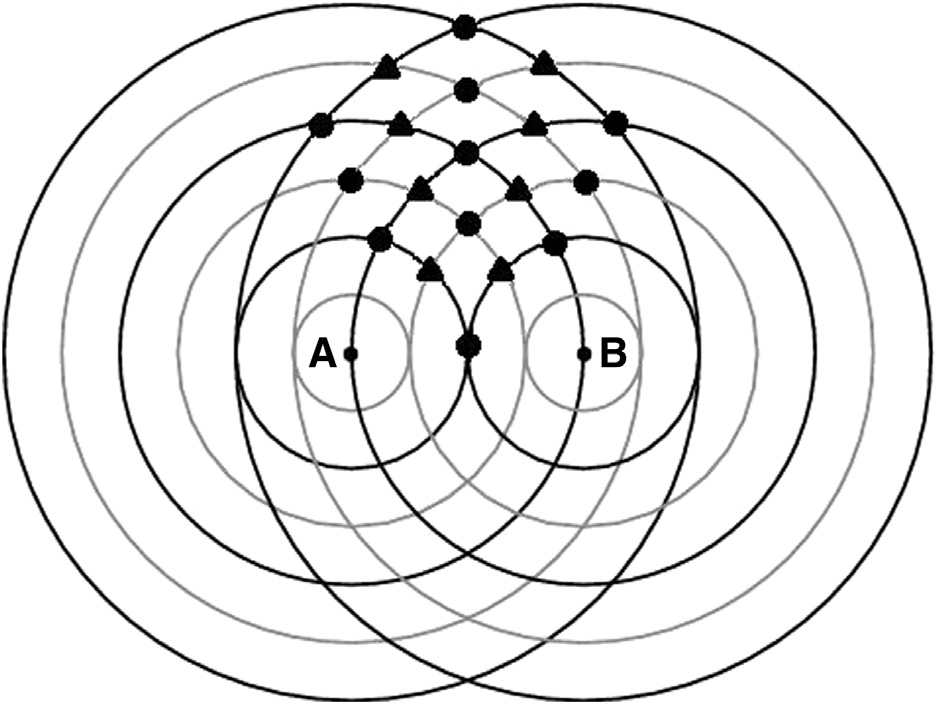
physics experiments have shown how waves interact
He brought the technique to his family and subse-
with each other: Depending on the pattern, some
quently opened a clinic to treat the public. Usui taught
waves are enhanced and some are cancelled ).
Reiki therapy level one to many people and taught sev-
The interference pattern between two human mag-
eral students the master/teacher level ().
netic fields may explain some of the results that any
Usui taught Reiki therapy as part of a spiritual practice,
touch therapy creates.
but not as a religion As Reiki therapy
The theory of quantum physics may hold promise
evolved and came to the West, the hands-on healing
in the future explanation of the mechanisms of Reiki.
practices came to the fore and the spirituality piece
Although no verified theory exists that explains how
of the practice faded. There are three degrees or levels
Reiki therapy (or any biofield energy therapy) works,
of Reiki practice. First degree practitioners are able to
a scientific explanation for Reiki therapy may be found
treat themselves or others through light touch
in quantum physics, a branch of physics that was first
This level of Reiki is suitable for anyone
discovered in the 1800s and studies extremely small
from school aged children to the very old. Second de-
particles (electrons, photons, and the like) that do
gree Reiki expands practice to the use of distance heal-
not behave in a predictable way. Quantum physics
ing: the practitioner may send Reiki energy to the next
studies these particles and attempts to describe the in-
room or around the world (). Third degree
teractions of energy and matter. Physicists have found
or master level Reiki expands Reiki practice to teach-
that very tiny particles have some very curious proper-
ing and initiating others into Reiki and involves exten-
ties. Not only can these tiny particles be in more than
sive practice.
one place at one time, some theorists say they must be
A typical Reiki therapy session can last from 30 to
in more than one place at the same time (
90 minutes. Ideally, the recipient lies comfortably on
). The Nobel Prize in Physics for 2012
a massage table fully clothed and the practitioner pla-
was won by two scientists who were each able to de-
ces their hands lightly on the body in a set sequence
tect a particle being in two places at the same time
Effect of Reiki Therapy
These particles by definition are difficult to mea-
sure, but beginning in the 1960s, scientists began mea-suring the biomagnetic field coming from the humanheart, which is believed to extend beyond the body(). In the 1990s Dr. John Zimmerman was ableto measure a biomagnetic field coming from a healingpractitioner's hands ) with a device calleda
(SQUID). A few years later, a Japanese team measureda biomagnetic field emanating from the hands of prac-titioners of yoga, meditation, Qigong, and similar mo-dalities (). These electromagneticsignal pulses varied from 0.3 to 30 Hertz (cycles persecond). Device-generated pulsed electromagneticfields (PEMF) have been effective for bone stimulation,
FIGURE 1. - Wave interference pattern. (A) and (B) repre-
stroke rehabilitation, decreased postoperative pain,
sent two people standing near each other. The black lines
and other applications
represent peaks, and the grey lines represent troughs. The
circles indicate areas where the two waves enhance each
electrical nerve stimulation (TENS) units are a well-
other (either higher peak or lower trough). The diamonds
known example of an adjustable pulsed electromag-
indicate areas where the two waves cancel each other.
netic field that is used to decrease chronic pain.
Although it may be difficult to imagine tiny particles
(Biofield energy may be gath-
that react to human thought, scientific experiments
ered and directed by the practitioner to the recipient
have shown this phenomenon to be true for some
as explained by quantum physics, e.g., thought pro-
time now (The similarities between
duces change in how the particles work (
human-generated biomagnetic energy, such as Reiki
). Distance healing may be explained
therapy, and device-generated electromagnetic fields
by energy particles being simultaneously present at
for healing seem clear. The measurement of human
the location and time of the Reiki practitioner and
biofield energy demonstrates the existence of human-
the location and time of the recipient through the in-
generated biomagnetic energy. The similarities in the
tention of the Reiki practitioner.
behavior of quantum particles and Reiki energy require
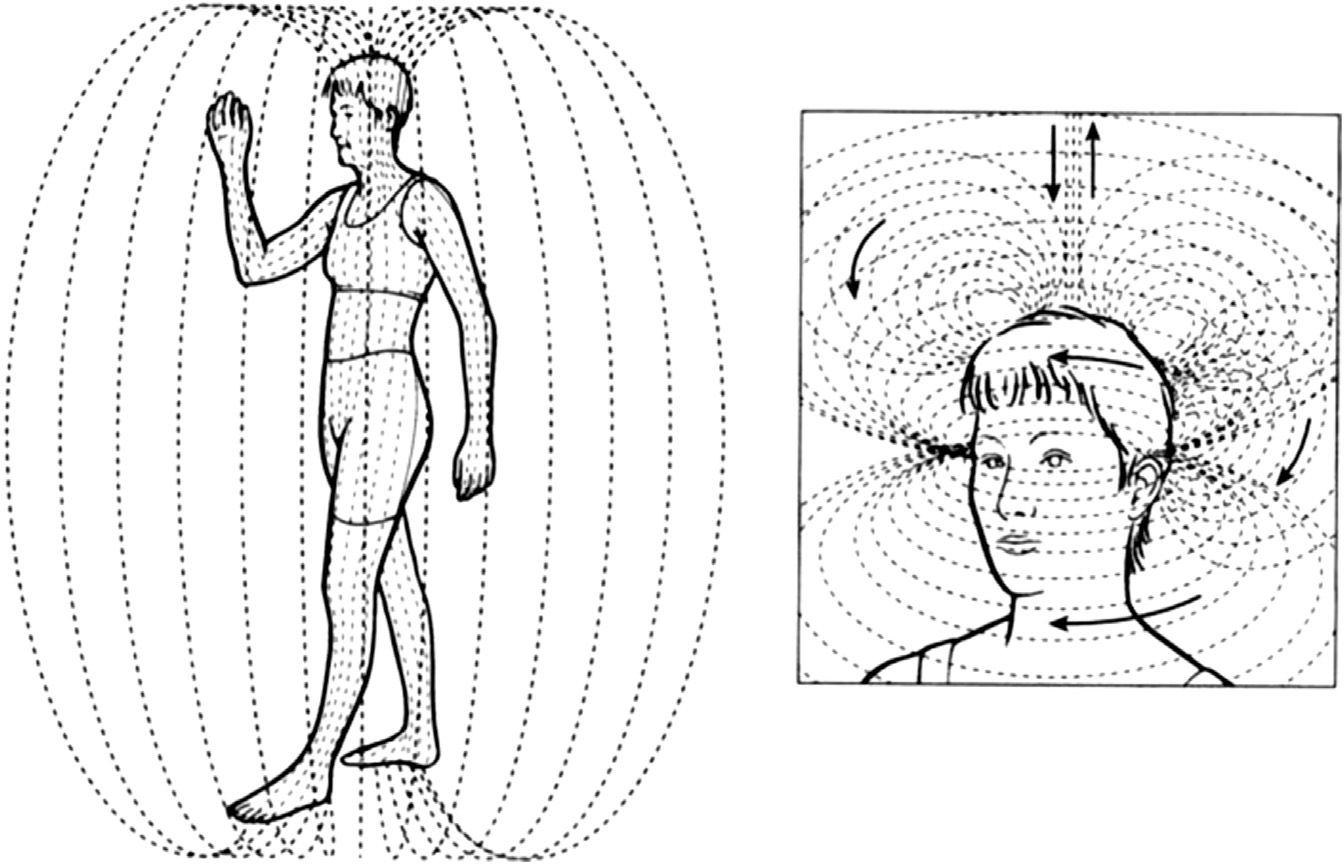
FIGURE 2. - Human biofield as it extends outside the body. Reprinted from Energy Medicine: The Scientific Basis (Ó2000),with permission from Elsevier Limited (J. L. Oschman, Polarity, therapeutic touch, magnet therapy, and related methods,p. 77).
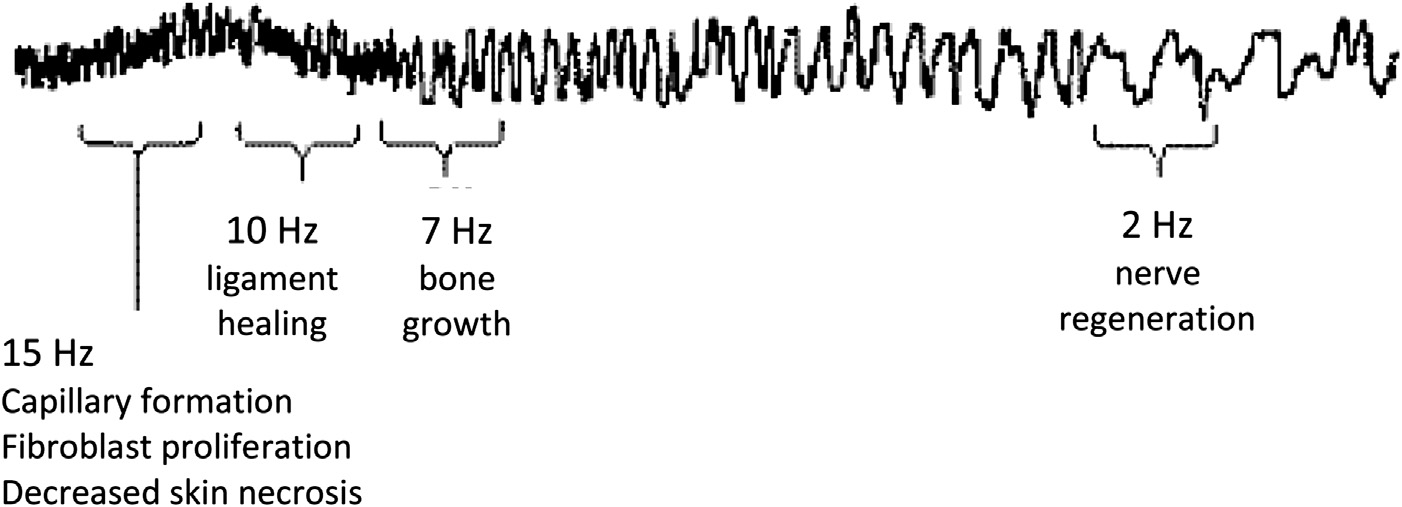
FIGURE 3. - Signal recorded from the hands of a therapeutic touch practitioner on the SQUID device. Reprinted from EnergyMedicine: The Scientific Basis (Ó2000), with permission from Elsevier Limited (J. L. Oschman, Polarity, therapeutic touch,magnet therapy, and related methods, p. 79.
more study; however, repeated physics experiments
used: pain, anxiety, and Reiki. The last search was
with thought-driven particles united with the measure-
run on April 4, 2012. After removing duplicates, there
ment of human biofield energy suggests that Reiki en-
were 49 articles: 17 review articles, 6 informational ar-
ergy may consist of quantum particles that may lead to
ticles, 1 study that reported on the prevalence of CAM
a validated theory of Reiki therapy.
use that included Reiki, 6 qualitative studies, 1 disserta-tion, and 18 studies of any type, any year.
Studies that include Reiki therapy as an interven-
tion are scarce. To present the best evidence, articles
Pain is a very common symptom. Approximately 100
were included in the review if they (a) used Reiki ther-
million Americans suffer from chronic pain (
apy as one arm of the study, (b) used randomization
). Additionally, millions of people suf-
with a control or usual care group, (c) were published
fer from acute pain (pain that lasts for 6 months or
in peer-reviewed journals, (d) measured either pain or
less), such as people with cancer or trauma and surgi-
anxiety, (e) were published in 2000 or later, and (f)
cal patients, and others suffer everyday events, such as
were published in English. After evaluating the 18 stud-
a sprained ankle or a stubbed toe. Anxiety is a state that
ies against inclusion criteria, 12 studies remained for
can accompany many of the conditions that cause
pain, such as with the diagnosis of a serious illness(e.g., cancer or heart disease).
Very few high-quality studies have explored Reiki
METHOD OF REVIEW AND DATA
therapy for pain and anxiety. Despite the lack of evi-
dence, articles are published in peer reviewed journalsgiving anecdotal evidence for the effectiveness of Reiki
Each of the 12 studies selected for full text review was
therapy and citing the few studies that have been pub-
carefully evaluated by both authors against the inclu-
sion criteria. Five of the 12 did not fully meet the inclu-
). Although four review articles have been
sion criteria. One article was a one-page preliminary
published that examined Reiki therapy in clinical
report (a second used a convenience sam-
ple with no randomization or control
), a third used a semi-randomized patient prefer-
), none focused exclusively on pain and anxiety
and none report effect sizes for study variables.
a fourth used a four-group design with a combinationof Reiki and sham Reiki and no control
SEARCH STRATEGY AND INCLUSION
and the fifth in-
cluded a control group that was different from thestated design and the two experimental groups
A systematic search was conducted using PubMed, Pro-
Quest, Cochrane, PsychInfo, CINAHL, Web of Science,
seven studies met the inclusion criteria for review as
Global Health, and Medline databases in addition to the
determined by both authors (
Center for Reiki Research (
). The following key words were
Effect of Reiki Therapy
FIGURE 4. - Article flow diagram.
cancer patients (
), two tested Reiki therapy in
Data were extracted from each study, including (a)
a surgical setting
sample population (disease process, gender, mean age,
), and two looked at Reiki therapy in adults
and race if available), (b) study design, (c) outcome
living in the community (
measures for anxiety or pain or both, and (d) statistical
). The results from each
significance for within group and between group dif-
individual study are shown in
ferences including p values, means, standard devia-tions, and z values for calculating Cohen's d statistic
Study Design and Comparison Groups
for effect sizes.
All studies in this review used randomization as speci-fied in the inclusion criteria. Three studies used a two-
group design, with the control group utilizing eitherusual care or
Sample sizes for the seven studies included in this re-
wait list control ().
view ranged from 16 to 160 participants (median ¼
used a rest period equal to the Reiki therapy in-
24) for a total of 328 participants. There were 48%
tervention as the control group, and
women and the mean age for the overall sample was
used a random crossover design. Two studies used
63 years old. Only two studies mentioned race.
a three-group design. explored Reiki
had 91% white participants but did not
therapy compared with Relaxation Response Therapy
say how the remaining 9% of the participants identified
(RRT) and a wait list control, and
themselves. reported 75% white,
explored Reiki and sham Reiki compared with usual
13% Asian, and 12% other participants.
care. In sham Reiki, an actor performs the same treat-
The seven studies included in the review
ment sequence as the real Reiki practitioner, but
examined a variety of populations: three studied
with no Reiki energy.
TABLE 1.
Summary of Reiki Studies
Examine the clinical
Anxiety/Reiki: twice
Prostate cancer: 54
Y Anxiety for RRT
effects of RRT and
adult males, mean
(p ¼ .02)
Reiki vs. control
age 64 years (range
Y Anxiety for Reiki
� Wait-list control
46-91), 91% white
(p ¼ .10)
RRT: Reiki (p ¼ .02)
d ¼ .57†
(p ¼ .01)
d ¼ .62†
Determine whether
Pain/Reiki treatments
Randomized to either
Cancer, primarily
Reiki þ standard
on days 1 and 4 of
Reiki or rest group
opioids resulted in
a 7-day trial for 90
(p ¼ .035)
d ¼ .64†
better pain control,
less analgesic use
(p ¼ .002)
d ¼ .93†
and improved QOLwhen compared
with opioid þ rest
Examine the effects
Pain, Anxiety/One
Cancer: 16 adults
of Reiki on fatigue,
Reiki treatment for
pain, anxiety, and
5 consecutive days
last Reiki session:
overall quality of life
15.23) 81% female,
Y Pain (p < .05)
in cancer patients
week washout then
Y Anxiety (p < .005)
2 Reiki treatment
the following week
with a diagnosis of
(3 weeks total) for
colorectal (63%),
d ¼ .32†
d ¼ .64†
gastric (12%), or
(no p values given)
lung (12%) cancer
Determine feasibility
Randomized to either
Reiki: HADS (anxiety)
of testing Reiki for
treatment within 7
Reiki or usual care
cancer: 32 women,
Usual: HADS (anxiety)
treatment within 7
days after biopsy
between groupmeans.
Compare levels of
Pain, Anxiety/Reiki
Randomized to either
Reiki: Usual Care
Reiki or usual care
Y Pain at 24 hours
40-73 years (mean
(p ¼ .04)
d ¼ .79†
op, 24 hours and 48
¼ 47, SD ¼ 6.5)
Y Anxiety (p ¼ .005)
d ¼ 1.36†
hours post-op for
Y Pain medication
Y Dilaudid time 2
(p ¼ .001)
d ¼ 1.82†
Y Dilaudid time 3
(p ¼ .007)
d ¼ 1.29†
(p ¼ .04)
d ¼ .81†
Type 2 diabetes 160
Y total pain (p ¼ .002)
� Sham Reiki (88)
alleviate pain and
� Usual care (26)
Y total pain (p ¼ .039)
improve mobility in
subjects with Type
Y total pain (p ¼ .622)
differencesbetween groups for
Evaluate the effect of
Pain, Anxiety/Reiki
Randomized to either
treatment once per
experiment or wait
20 adults ages 57
Y Pain (p ¼ .0078)
list control group
Y Anxiety (p ¼ .0005)
63.8 (SD ¼ 4.9),
[ Pain (p ¼ .0156)
[ Anxiety (p ¼ .0313)
d ¼ 4.5†
d ¼ .75†
pain, depression,and/or anxiety
*Within group differences.
†Between group differences.
TABLE 2.
Summary of Results: Reiki Therapy and Control Groups
Sham Reiki, Usual
Care, Waitlist Control,
Time 1 ¼ 7.29 (4.80)
Time 1 ¼ 8.27 (5.16)
Time 3 ¼ 6.18 (4.60)
Time 2 ¼ 5.73 (5.15)
24 hours postsurgery
24 hours postsurgery
Post ¼ 2.2 (1.2)
Post ¼ 7.6 (1.2)
Pre ¼ 25.2 (14.4)
Pre ¼ 21.2 (12.9)
Post ¼ 17.5 (15.5)
Post ¼ 28.5 (13.5)
Diff ¼ difference; RRT ¼ Relaxation Response Therapy.
Variables and Measures
unspecified ‘‘Likert'' scale to measure pain.
Three of the studies examined both pain and anxiety
also used the ESAS questionnaire men-
tioned above to evaluate pain.
Two studies considered just pain
used The McGill Pain Questionnaire )
to evaluate pain in patients with painful diabetic neu-
only evaluated anxiety
ropathy. used the FACES pain
). There were a variety of validated measures used.
scale that was originally developed for children but
Anxiety. Three studies chose the Spielberger State
that has been shown to be effective in older adults
to measure anxiety
(). The STAI scale was originally created to
Outcomes and Effect Sizes
measure anxiety in adolescents with cancer but has
All but one study included in this review achieved at
been well validated in adults.
least one statistically significant result on the outcome
used the Edmonton Symptom Assessment System
variables of interest for the Reiki therapy intervention.
(ESAS) questionnaire (
Effect sizes were calculated using standard equations
), a validated nine-symptom visual analog scale
and were measured using the Cohen's d statistic. Effect
to measure anxiety. Potter also used the Hospital Anx-
sizes for the Reiki therapy intervention ranged from
iety and Depression Scale (HADS) (
small (d ¼ .28) to very large (d ¼ 1.82).
), because it recognizes anxiety in populations
Anxiety. While investigating Reiki therapy and relaxa-
suffering from physical symptoms as a result of their
tion response therapy compared with wait-list control
disease. used the HAM-A rating
for men with prostate cancer receiving radiation ther-
scale, which exhibits high reliability and internal con-
apy, found a within group decrease
sistency (Cronbach's alpha ¼ .85, r ¼ .23, p < .05)
in anxiety for relaxation response therapy (RRT) with
a medium effect size (p ¼ .02, d ¼ .55) and a nonsignif-
Pain. Two studies used an 11-point Visual Analog
icant within group decrease in anxiety for Reiki therapy
with a small effect size (d ¼ .39). The between group dif-
ferences of RRT compared with Reiki therapy resulted
Effect of Reiki Therapy
in a significant difference between RRT and Reiki ther-
when calculated using means and standard deviations
apy (p ¼ .02, d ¼ .57) and between RRT and control
(p ¼ .01, d ¼ .62) both in favor of the RRT intervention.
investigated the effect of Reiki therapy on
Working with cancer patients who had recently com-
pain in women after hysterectomy, the study found
pleted chemotherapy treatment,
a significant between group decrease in pain at 24
found within group differences for a decrease in anxiety
hours postsurgery (p ¼ .04) and a borderline large ef-
(p < .005) and a large effect size (d ¼ .83) for subjects in
fect size (d ¼ .79). Of equal interest, comparing the Re-
the Reiki therapy treatment arm when measured before
iki therapy and usual care groups, the women in the
the first Reiki therapy treatment compared with after
Reiki therapy intervention took less pain medication
the last Reiki therapy treatment in a group of cancer pa-
at time 2 (p ¼ .001, d ¼ 1.82), time 3 (p ¼ .007, d ¼
tients on standard opioid therapy. When comparing Re-
1.29), and time 6 (p ¼ .04, d ¼ .81) with large to
iki therapy versus rest for between group differences,
very large between group effect sizes. In a study to ex-
there was a medium effect size (d ¼ .64) when calcu-
plore the effect of Reiki and sham Reiki compared with
lated using means and standard deviations.
usual care for painful diabetic neuropathy,
found a nonsignificant within group decrease
found that Reiki and sham Reiki resulted
in anxiety with a small effect size for the HADS anxiety
in a within group decrease in pain (p ¼ .002 and p ¼
subscale for both the Reiki therapy intervention (d ¼
.039, respectively) and a small effect size (d ¼ .36
.24) and the usual care group (d ¼ .24) and for the
and d ¼ .26, respectively), while the usual care group
STAI measure for the Reiki intervention (d ¼ .27) and
had a nonsignificant within group decrease in pain and
the usual care group (d ¼ .49) when exploring the
a very small effect size (p ¼ .622, d ¼ .17). There were
use of Reiki therapy for women undergoing a breast bi-
no between group differences in total pain. Comparing
opsy. There were no between group differences when
a Reiki therapy intervention with a wait list control
comparing the Reiki therapy intervention to usual
group of community dwelling older adults, there was
care. In an investigation of women undergoing hyster-
a significant within group decrease in pain (p ¼
ectomy, found a significant between
.0078) and a large effect size (d ¼ 2.08) and a significant
group decrease in anxiety (p ¼ .005) and a large effect
within group increase in pain (p ¼ .0156) and a large
size (d ¼ 1.36) just before discharge from the hospital.
effect size (d ¼ �2.08) for the wait list control group
found a significant decrease in
(Because of the decrease in
anxiety (p ¼ .0005) and a large effect size (d ¼ 2.08)
pain for the Reiki therapy group and corresponding in-
within the Reiki therapy intervention and a significant
crease in pain for the control group, the calculated ef-
increase in anxiety (p ¼ .0313) and a large effect size
fect size for the between group difference was very
(d ¼ �.208) within the control group while investigat-
large (d ¼ 4.5).
ing the use of Reiki therapy with community-dwellingolder adults. When calculating between group differ-
ences after Reiki therapy intervention, there wasa very large between group difference when comparing
Reiki therapy has been explored in a variety of popula-
the Reiki therapy group with the control group (d ¼
tions, including cancer patients, community dwelling
adults, and surgical patients. The studies included in
Pain. A Reiki therapy intervention used with cancer
this review exhibit design flaws common to research
patients found a significant between group decrease
involving complementary therapies. The most obvious
in pain (p ¼ .035) and a medium effect size (d ¼ .64)
difficulty is sample size. The median number of study
on day 1 of the intervention and a significant between
participants was 24 (range of 16 to 160 participants).
group decrease in pain (p ¼ .002) and a large effect size
It is difficult to make generalizations to a population,
(d ¼ .93) for opioids plus Reiki therapy when com-
even a limited one such as adults with cancer, using
pared with opioids plus rest on day four of the inter-
such small sample sizes. Moreover, acquiring these
vention (Cancer patients in the
samples may take months to years. For example,
() study who had recently completed
took 22 months to recruit 54 sub-
chemotherapy realized a significant decrease in pain (p
jects, and Potter required 15 months to recruit 32 sub-
< .05) and a medium effect size (d ¼ .76) for within
group measures when comparing scores from before
difficulties if a longitudinal design would be more ap-
the first Reiki treatment with the scores from after
propriate. had difficulty recruiting
the final Reiki treatment. When comparing between
subjects and, in fact, took 2 years to recruit 24 adults
group scores for Reiki therapy versus rest, the Reiki
because the subjects stated they would not participate
therapy group realized a small effect size (d ¼ .32)
unless they could be in the Reiki therapy group.
also had to limit the control
placement and timing protocol, making it difficult to
group because of high attrition.
compare subjects to each other much less compare be-
Length of intervention may have been problem-
tween studies.
atic for some study outcomes. Although was able to show a significant reduction in
Suggestions for Future Research
pain and a medium effect size for the Reiki treatment
Based on the findings of this review, it may be helpful if
group (p ¼ .035, d ¼ .64) on day 1 and significant re-
future Reiki therapy studies consider the following de-
duction in pain and a large effect size on day 4 (p ¼
sign strategies. First, to be able to conform to scientific
.002, d ¼ .93), the intervention consisted of only two
research standards, a three-arm design that includes
Reiki treatments 4 days apart. It seems possible that
a Reiki intervention, a sham Reiki intervention (pla-
if the study had lasted several weeks they may have
cebo), and a nonintervention control group seems
seen the decrease in medication usage that they were
most effective. Having a sham Reiki group allows for in-
looking for. Another study that may have benefitted
vestigators to take into account and control for the ther-
from a longer intervention time was
apeutic effect of attention and potential effect of human
when they examined Reiki therapy for reduc-
interaction. It has been shown that any touch therapy,
tion in pain in diabetic subjects with painful diabetic
even a sham intervention produces an effect on sub-
neuropathy (PDN). Although this was one of the longer
jects, as reported by several of the studies in this review.
interventions (12 weeks total), PDN is not an easy con-
Reiki interventions need to show significantly better re-
dition to treat and does not respond well to medica-
sults than the sham group to overcome the ‘‘placebo ef-
fect.' It is suggested that effect sizes be calculated and
a statistically significant decrease in pain for the Reiki
reported in articles so that readers can understand
group (p ¼ .002, d ¼ .36), the effect sizes were not
and compare the effect of the interventions. Second,
very different for the sham Reiki group (p ¼ .039,
to combat the reluctance of subjects to participate in
d ¼ .26) leading the authors to question the clinical sig-
complementary research, a crossover design is sug-
nificance. Possibly if the intervention had run 26
gested. In this way, control subjects know that they
weeks or longer, the authors may have been able to de-
will receive the intervention either now or in the near
tect a difference between the Reiki group and the
future. Studies that use a crossover design seem to
sham Reiki group.
have fewer issues with control groups
Timing of interventions also can be important to
Third, a standardized
success. For example, in the Reiki therapy intervention
protocol of intervention length and hand positions
for breast biopsy, the pre-biopsy intervention was
seems essential. It is difficult to compare subjects who
given within 7 days before the biopsy and the post-
have not used the same treatment protocol. Fourth,
biopsy intervention was given within 7 days after the
researchers need to consider whether Reiki therapy
biopsy. The study author admitted that the timing
is appropriate for a particular condition and what the
was for subject convenience and that an intervention
optimal timing of the intervention may be. For
‘‘within the clinical setting might more effectively mit-
example, the timing of the Reiki treatments used
igate a crisis response'' (p. 246). In con-
in the abdominal hysterectomy study (
trast, timed the Reiki
consisting of immediately before sur-
therapy intervention around abdominal hysterectomy
gery then 24 hours and 48 hours after surgery, was
in a way that makes more sense: just before surgery,
well considered and makes sense.
then 24 hours and 48 hours after the surgery. This tim-
Another possible avenue of research would be to
ing resulted in a significant decrease in both pain and
teach first degree Reiki to subjects and have them prac-
medication usage.
tice Reiki therapy as a self-healing strategy. This could
Most studies included in this review used a stan-
be combined with weekly or periodic Reiki treatments
dardized protocol of timing and hand positions. How-
by a Reiki therapy professional. The reasons for this sug-
ever, these protocols differed significantly from study
gestion are two-fold. First, a preliminary report using
to study. Reiki treatment times varied from 25 minutes
this method with an HIV population showed a decrease
in the diabetic neuropathy study ()
in pain and anxiety using self-Reiki (). Sec-
to 90 minutes in the Reiki therapy plus opioid use in
ond, when considering the study using Reiki versus
cancer patients study (). The average
RRT for men with prostate cancer, the RRT arm showed
treatment length was 48 minutes. All but one study
a larger decrease in anxiety This
used a set protocol for treatment hand positions.
may be because the men using RRT were encouraged
allowed the treatments to be pa-
to practice daily while the Reiki therapy intervention
tient specific rather than follow a particular hand
was only twice per week. It would be interesting to
Effect of Reiki Therapy
discover whether daily Reiki self-treatment would pro-
difficult to recruit subjects into nondrug-related stud-
duce a larger decrease in pain or anxiety than a once
ies, more than one study specifically mentioned the
or twice weekly session given by a Reiki therapy
difficulty of recruiting or keeping subjects in the non-
Reiki control groups.
On the other hand, most studies in this review did
achieve statistical significance or near significance on
Every effort was made to limit bias in study selection.
the variable of interest; either pain or anxiety or
Inclusion criteria were tight and strictly adhered to.
both. Effect size calculations were performed using Co-
Small sample sizes may contribute to some inflation
hen's d, which allows comparison of studies in a stan-
of effect sizes. Only studies that used a reliable random-
dardized way. Effect sizes for most of the studies in this
ization scheme were included. There was no require-
review went from small to very large. Based on statisti-
ment on study use of validated measures, although
cal significance, the strength of the effect sizes
most studies included in this review did use validated
(and public interest in Reiki therapy as a non-
measures. Only studies published in English were in-
invasive and even comforting intervention, there is
cluded, and no gray literature such as dissertations or
enough evidence to suggest continued research using
conference abstracts were included. Publication bias
Reiki therapy. Suggestions for study design and stan-
may, of course, account for some inflation of results.
dardization of treatment protocol were proposed to in-crease the potential for positive outcomes in future
There are very few high quality studies that explore the
Implications for Nursing Education, Practice,
use of Reiki therapy for pain or anxiety. Because the
number of studies is small, the interventions are dis-
Reiki therapy is a noninvasive, often comforting, and
similar from each other, and the populations presented
relaxing intervention that is within nursing scope of
are so different, it is difficult to make generalizations or
practice in most states. Nurses may easily learn Reiki
recommendations from these studies. Some of the dis-
therapy and use this intervention with patients in
similarities include length of individual treatments,
day-to-day practice (Addi-
which ranged from 30 to 90 minutes, and population
tionally, Reiki therapy may be a good self-care tool, as
variations, which varied from cancer patients to surgi-
suggested by more than one study (
cal patients to community dwelling adults. Design
issues included small sample sizes, the timing of inter-
Based on this review, there is enough evidence to
ventions in relation to the complaint, and the length of
continue researching Reiki therapy as an intervention
the intervention in relation to the issue being ad-
for pain and anxiety. Certainly more research is
dressed such as painful diabetic neuropathy, which is
required to definitively recommend Reiki therapy as
known to be difficult to treat. Although it is often
an intervention for decreased pain or anxiety.
Rae, A. I. M. (2005). Quantum Physics: A beginner's guide
Institute of Medicine. (2011). Relieving pain in America: A
blueprint for transforming prevention, care education, and
research. Retrieved April 23, 2012 from
The International Center for Reiki Training. (2012).
The Center for Reiki Research. Retrieved April 9, 2012 from
Thomas, A. D. H. (2012). Hidden in plain sight: The simple
link between relativity and quantum mechanics. Swansea,
UK: CreateSpace Independent Publishing Platform.
National Center for Complementary and Alternative
Medicine. (2012, July 2009). Reiki: An introduction. Re-
trieved April 22, 2012 from
Nobelprize.org. (2012). The nobel prize in physics 2012,
Source: https://sireiki.co.uk/wp-content/uploads/2016/07/1-s2.0-S1524904213000805-main.pdf
Supporting pupils at school with medical conditions Statutory guidance for governing bodies of maintained schools and proprietors of academies in England December 2015 About this guidance This document contains both statutory guidance and non-statutory advice. The non-statutory advice is presented in text boxes.
A BETTER WAY Avoid treatment linked to the increasing Parkinson's disease death rate.™* *Hinz, M. Stein, A. Cole, T., The Parkinson's disease death rate: carbidopa and vitamin B6 (PLP) Clin Pharmacol Sep 2014 THE APPROACH Receive Parkinson's care developed by the medical doctors that discovered and published, the carbidopa death link.







