Washingtonmidwives.org
MIDWIFERY CARE FOR
EARLY PREGNANCY LOSS:
OPTIMIZING CLIENT CENTERED
COUNSELING AND MANAGEMENT
Tara Cardinal, CNM, ARNP
Marnie Raelene, MSM Student
Midwives Association of Washington State
2015 Spring Conference
ACKNOWLEDGEMENTS
Washington State Department of Health
Polly Taylor, CNM, MPH
Training, Education and Advocacy in Miscarriage
Sarah Prager, MD, MAS
Innovating Education in Reproductive Health
Robin Wallace, MD, MAS
Karen Hays, DNP, CNM, ARNP
Emily Godfrey, MD, MPH
Kristin Swanson, RN, PhD, FAAN
Linda Prine, MD
Differentiate between and list 3 different
classifications of spontaneous abortion
Describe 3 outpatient management options for
miscarriage management
Describe success rates of the 3 management
options based on type of early pregnancy loss diagnosis
Name 3 strategies to empower and support those
who are experiencing pregnancy loss
Identify 3 elements of the new Practice Guideline
for Washington State Midwives that optimize client-centered counseling and care.
Standard of Practice
Capacity and Limitations
Reinforcing your foundation
REVIEW: NORMAL IMPLANTATION & DEVELOPMENT
Implantation
5-7 days after fertilization
Takes 72 hours
Invasion of trophoblast
Embryonic disc
1 week post-implantation
If no embryonic disc,
trophoblast still grows but no embryo (anembryonic pregnancy)
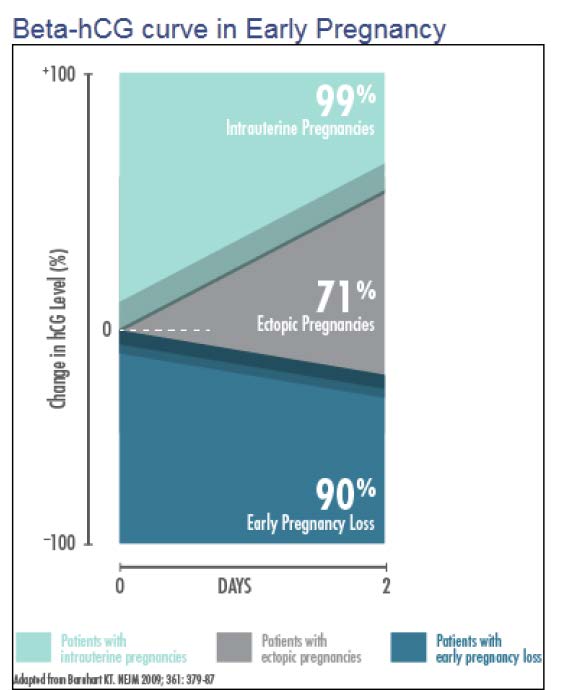
ßhCG Guidelines
Normal pregnancy
Spontaneous abortion
Ectopic pregnancy
Molar pregnancy
Twin pregnancy
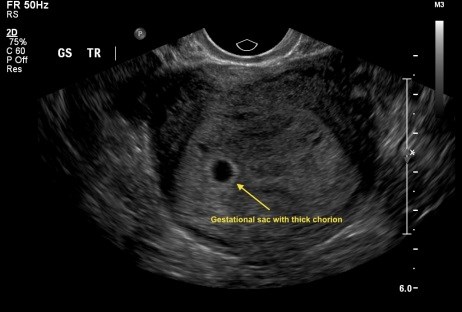

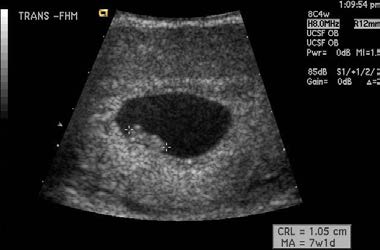
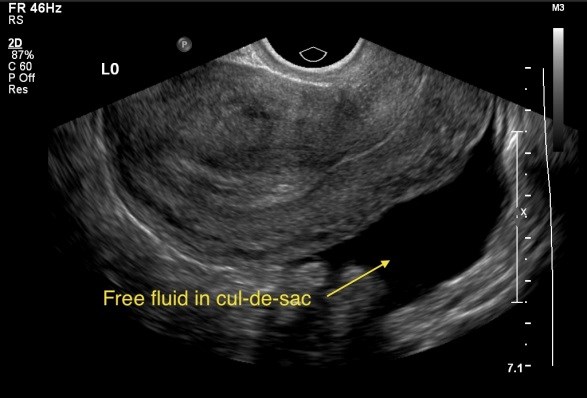
ULTRASOUND ASSESSMENT
innovating education in reproductive health - http://www.innovating-education.org/professionalism/managing-early-pregnancy-loss/evaluation-and-diagnosis/
Implantation anywhere other than
main uterine body
includes corunal, cervical, intra-
Adnexa are most common location
Anywhere there is sufficient blood
Can be difficult to diagnose
Managed expectantly, with
medication or operatively


DIFFERENT DIAGNOSIS SAME MEANING?
Spontaneous Abortion (SAb) most common
complication of early pregnancy
8-20% clinically recognized pregnancies
13-26% all pregnancies
800,000 SAb's estimated each year in the
80% of SAb's occur in 1st trimester
(Cunningham, et al. 2013; Prine et al, 2011; Prager, 2013)
Live Birth
End of 1st Trimester
Recognized Pregnancies
30% Pre-clinical
30% Implantation Failure
Brown S, Miscarriage and its associations. Sem Repro Med.
What did this pregnancy mean to your client?
What is their support system like?
What are their and their partner's individual needs?
How can they meet them together and separately?
Normalizing emotions
Empower them with information and options
What are their plans for future pregnancy? How will
they prevent another pregnancy until they are
emotionally ready?
(Prine, 2011; Swanson, 1999; Wallace, 2010)
FUTURE MISCARRIAGE RISK
NATURAL HISTORY OF MISCARRIAGE
33% anembryonic
50% due to chromosomal abnormalities
Host factors
Paternal factors?
(Cunningham, et al. 2013; Prager, 2013)
CLINICAL PRESENTATION OF EPL
Pain/cramping
Falling or abnormally rising
Decreased symptoms of
Pregnancy tissue
No symptoms at all!
(Cunningham, et al. 2013)
ULTRASOUND FINDINGS OF EPL
Anembronic Pregnancy
No fetal pole with mean
sac diameter 16-25 mm
Embryonic Demise
(Mishell , 2007)
MANAGEMENT OPTIONS
Expectant Management
Medical Management
Procedural Management
MVA/EVA/D&C in the OR
Most often with general anesthesia
(Godfrey, 2009; Prine, 2011)
PATIENT PREFERENCE AND SATISFACTION PATIENTS DEMONSTRATE HIGHEST LEVELS OF SATISFACTION WHEN THEY ARE COUNSELED ON ALL OF THE MANAGEMENT OPTIONS AND ABLE TO CHOOSE THE METHOD THAT IS RIGHT FOR THEM.
COUNSELING STEPS
Verbal and written instructions
Rule out ectopic
Recommendation for Rhogam
Provide contact information
Warning signs
Indicators of completion
EXPECTANT MANAGEMENT
*Candidates: *<13 weeks gestation *by sure, regular LNMP or US *Stable vitals *No evidence of infection *No increased risk of excessive bleeding *Rule out ectopic and molar *Willing to have aspiration if complications arise
EXPECTANT MANAGEMENT
Wait for pregnancy to miscarry naturally
Can take 1-2 months
Bleeding should lighten and lessen after 3-5 hours of
May elect medication or aspiration option at any time
May not complete naturally and need aspiration
Check in by phone during expectant period
Recommend 1-2 week follow up after complete
WHAT IS SUCCESS?
Definitions used in studies
≤ 15 mm endometrial thickness (ET) 3 days to 6
weeks after diagnosis
No clear rationale for this cut off
No vaginal bleeding
Negative urine ßhCG
Absence of gestational sac
(Harwood, 2001; Reynolds, 2005)
WHEN TO INTERVENE FOR EXPECTANT MANAGEMENT?
Continued gestational sac
Clinical symptoms
Patient preferences
When not to intervene:
Vaginal bleeding and positive UPT are possible for 2-
Poor measures of success
MEDICATION MANAGEMENT
Prerequisite for treatment
<13 weeks gestation
Stable vital signs
No evidence of infection
No allergies to medications used
Adequate counseling and patient acceptance of side
Aspiration if complications arise
MEDICATION MANAGEMENT
Increases uterine contractility and cervical softening
Prostoglandin E1 analogue
Not FDA approved specifically for EPL
Used off-label for many OB/GYN indications
Designated essential medication by WHO
Mifepristone & Misoprostol
Methotrexate & Misoprostol
MEDICATION MANAGEMENT
Patient can take 1-2 doses 800 mcg misoprostol to
accelerate miscarriage (12-24 hours apart)
Can control timing to a degree
Expected to complete within 24 hours after miso
May elect aspiration at any time
Medication effective 90% of the time, may need
additional dose of medication or aspiration to complete
Recommend 1-2 week follow-up
MISOPROSTOL BY ROUTE OF ADMINISTRATION
Serum Level Comparison
Uterine Activity Over 5 Hours
Buccal - Meckstroth
Sublingual - Tang
ctivity (A 1000
Time (min)
(Meckstroth et al., 2006)
SIDE EFFECTS AND COMPLICATIONS
Misoprostol vs. Placebo
Nausea, vomiting, and diarrhea – increased with miso
Pain – increased analgesics
Hemoglobin Concentration – no difference
Infection: 0% for placebo vs. 0.2-4.7% for misoprostol
No benefit with repeat dosing within 3-4 hours
Improved outcome with 1 repeat dose at 24 hours if
90% found medical management acceptable and would
elect same treatment again
Wood SL, Obstet Gynecol 2002; Bagratee JS, Hum Reproduct
2004; Blohm F, BJOG: Int J Obstet Gynecol 2005
MEDICATION MANAGEMENT: BOTTOM LINE
Medical Management
Misoprostol 800 mcg pv (or buccal) Repeat x 1 at 12–24 hours,
Occasionally repeat more than once
Infection prophylaxis:
Doxycycline 200 mg #1 or azithromycin 1g (500 mg x #2)
Pain control:
Ibuprofen 800 mg and advise PO q 6-8 hours PRN #30
Hydrocodone/acetaminophen 5/325 mg PRN #12
OR oxycodone/acetaminophen 5/325 mg PRN #12
Measure success as with expectant management
WHEN TO INTERVENE FOR MEDICATION MANAGEMENT?
Continued gestational sac
Clinical symptoms
Patient preferences
When not to intervene:
Vaginal bleeding and positive UPT are possible for 2-
ET >15mm and relatively homogenous
Poor measures of success
OUTCOMES
RATES OF SUCCESSFULLY COMPLETED MISCARRIAGE USING
EXPECTANT MANAGEMENT OR MISOPROSTOL BY SUBCATEGORY
OF EARLY PREGNANCY LOSS FROM DAY OF DIAGNOSIS:
Completed miscarriage with Misoprostol
EXPECTANT management
Subcategory By day 7
of EPL
Incomplete
abortion
Embryonic
demise
Anembryonic 25%
gestation
All categories 40%
(adapted from Luise, 2002 & Zhang, 2005)
UTERINE ASPIRATION
Who should have aspiration management:
Significant medical morbidity
Risk for heavy bleeding
Anyone who wants it
UTERINE ASPIRATION
Who is eligible for outpatient management:
<13 weeks gestation
Stable vitals
No evidence of infection
No increased risk of excessive bleeding
Rule out ectopic
BMI <50 and <350 lbs.
No uterine anomalies
Psychologically stable
refer severe anxiety for OR management
UTERINE ASPIRATION
UTERINE ASPIRATION
Actual aspiration procedure takes 2-5 minutes
Infection prophylaxis:
Doxycycline 200 mg #1 or azithromycin 1g (500 mg x #2)
Pain control:
Ibuprofen 800 mg and advise PO q 6-8 hours PRN #30
Hydrocodone/acetaminophen 5/325 mg PRN #12
OR oxycodone/acetaminophen 5/325 mg PRN #12
Ativan 2 mg x #2
STEPS FOR PERFORMING MVA
A step-by-step poster is
available from the manufacturer of a popular MVA device to guide clinicians through the procedure.
MVA COMPLICATIONS
MVA in the absence of contraindications and by
a trained provider is a safe procedure
MVA is 98-99% successful
Rare complications in first trimester
Risk of complications increase with advancing
Compared to complications in pregnancy
(Prager, 2013; TEACH, 2014; TEAMM, 2014)
ASPIRATION MANAGEMENT EARLY PREGNANCY LOSS
BENEFITS
Convenient timing
Infection (1/200)
Observed therapy
Perforation (1/2000)
High success rates
Uterine synechiae
POST-MISCARRIAGE CARE
Rhogam scheduled at time of diagnosis or procedure
Pelvic rest for 2 weeks
Initiate contraception upon completion of procedures
Expect light-moderate bleeding for 2 weeks
Menses return after 6 weeks
Negative ßhCG values after 2-4 weeks
Appropriate grief counseling and resources
(Goldstein, 2002; Prager, 2013; Wyss, 1994)
SCOPE OF PRACTICE
Who can do what to whom, in what settings and
under what conditions
Varies by state and country
Core foundation of
Individual education, experience, training
Professional organization standards
Legal and regulatory
EXPECTANT MANAGEMENT OF FIRST TRIMESTER MISCARRIAGE:
A PRACTICE GUIDELINE FOR LICENSED MIDWIVES IN WA STATE
Commonly used terms defined
Signs/Symptoms of early pregnancy loss
Management options & how to explain them to
Good candidates for EM
Contraindications for EM
Pros & potential Cons for EM
Routine clinical care for EM including
suggestions on office visits & phone contacts
Recommendations for ritual after loss
Follow up care
Complications that midwife & client should
Spectrum of expected & potentially complicated
Emotional support
Referral & co-management resources
Sample client handout explaining EM
Allopathic & CAM options
How long is too long for EM?
Much of the research followed the ‘2-week rule,' but
in the absence of complications, and a desire by the woman to continue expectant management, there is no time limit to waiting for the body to naturally expel a spontaneous first trimester miscarriage.
If the process of expelling the POC has not started by
8 weeks after diagnosis of a nonviable pregnancy then the client & midwife should review management options again. If menstrual periods have resumed, the miscarriage can be considered complete. If there is any question or confusion about this, an ultrasound could confirm completion.
COMPLICATIONS REQUIRING CONSULTATION & REFERRAL
Severe or prolonged emotional distess, depression
or grief reaction
Fever (>100.4F)
Uterine tenderness
Foul smelling discharge or blood
Hemorrhage (soaking more than 2 menstrual
pads in 1 hour, or passing several clots larger than a golf ball
Severe pain anywhere
Extreme pain not controlled by OTC pain
OTC & CAM OPTIONS
Suggestions of things to try for:
Pain management
Stress/Anxiety
Promoting expulsion
Training, Education & Advocacy in Miscarriage
Management (TEAMM):
Managing Early Pregnancy Loss modules:
Ipas US Start-up Kit for Integrating Manual
Vacuum Aspiration (MVA) for Early Pregnancy
Loss into Women's Reproductive Health-care
Services:
SELECTED BIBLIOGRAPHY
*Ankum, W. M. (2001). Regular review: Management of spontaneous miscarriage in the first trimester: an example of putting informed
shared decision making into practice. BMJ, 322(7298), 1343–1346. doi:10.1136/bmj.322.7298.1343
*Barnhart, K. T. (2009). Ectopic Pregnancy. New England Journal of Medicine, 361(4), 379–387. doi:10.1056/NEJMcp0810384 *Cunningham F, Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoffman BL, Casey BM, Sheffield JS. Prenatal Care. In: Cunningham F,
Leveno KJ, Bloom SL, Spong CY, Dashe JS, Hoffman BL, Casey BM, Sheffield JS. eds. Williams Obstetrics, Twenty-Fourth Edition. New York, NY: McGraw-Hill; 2013. http://accessmedicine.mhmedical.com.offcampus.lib.washington.edu/content.aspx?bookid=1057&Sectionid=59789146. Accessed December 8, 2014
*Dighe, M., Cuevas, C., Moshiri, M., Dubinsky, T., & Dogra, V. S. (2008). Sonography in first trimester bleeding. Journal of Clinical
Ultrasound: JCU, 36(6), 352–366. doi:10.1002/jcu.20451http://accessmedicine.mhmedical.com.offcampus.lib.washington.edu/content.aspx?bookid=1057&Sectionid=59789146. Accessed December 8, 2014
*Doubilet, P. M., Benson, C. B., Bourne, T., & Blaivas, M. (2013). Diagnostic Criteria for Nonviable Pregnancy Early in the First
Trimester. New England Journal of Medicine, 369(15), 1443–1451. doi:10.1056/NEJMra1302417
*Godfrey, E. M., Leeman, L., & Lossy, P. (2009). Early pregnancy loss needn't require a trip to the hospital. The Journal of Family
Practice, 58(11), 585–590.
*Luise, C., Jermy, K., May, C., Costello, G., Collins, W. P., & Bourne, T. H. (2002). Outcome of expectant management of spontaneous
first trimester miscarriage: observational study. BMJ (Clinical Research Ed.), 324(7342), 873–875.
*Meckstroth, K. R., Whitaker, A. K., Bertisch, S., Goldberg, A. B., & Darney, P. D. (2006). Misoprostol administered by epithelial routes:
Drug absorption and uterine response. Obstetrics and Gynecology, 108(3 Pt 1), 582–590. doi:10.1097/01.AOG.0000230398.32794.9d
*Miller, E., Decker, M. R., McCauley, H. L., Tancredi, D. J., Levenson, R. R., Waldman, J., … Silverman, J. G. (2011). A family planning
clinic partner violence intervention to reduce risk associated with reproductive coercion. Contraception, 83(3), 274–280. doi:10.1016/j.contraception.2010.07.013
*Paul, M., Lichtenberg, S., Borgatta, L., Grimes, D. A., Stubblefield, P. G., & Creinin, M. D. (Eds.). (2009). Management of Unintended
and Abnormal Pregnancy: Comprehensive Abortion Care (1 edition.). West Sussex, England: Wiley-Blackwell.
*Prager, S. (2013). Do nothing, do something, do surgery: Management of early pregnancy loss. Miscarriage Management Training
Initiative. Seattle, WA. Miscarriagemanagement.org
*Prine, L. W., & MacNaughton, H. (2011). Office management of early pregnancy loss. American Family Physician, 84(1), 75–82. *Swanson, KM. (1999). Research-based practice with women who have had miscarriages. Journal of Nursing Scholarship. 31(4), 339-345. *Varney, H. (2004). Varney's midwifery (4th ed.). Sudbury Mass.: Jones and Bartlett Pub. *Wallace RR, Goodman S, Freedman LR, Dalton VK, Harris LH. (2010). Counseling women with early pregnancy failure: utilizing
evidence, preserving preference. Patient Education and Counseling. In press.
*Zhang, J., Gilles, J. M., Barnhart, K., Creinin, M. D., Westhoff, C., & Frederick, M. M. (2005). A comparison of medical management
with misoprostol and surgical management for early pregnancy failure. The New England Journal of Medicine, 353(8), 761–769. doi:10.1056/NEJMoa044064
Expectant Management of First Trimester Miscarriage:
A Practice Guideline for Licensed Midwives in WA State
Written by Marnie Raelene
Table of contents: I.
DIAGNOSIS OF EARLY PREGNANCY LOSS
MANAGEMENT OPTIONS FOR EARLY PREGNANCY LOSS
CANDIDATES & CONTRAINDICATIONS FOR EXPECTANT
PROS & CONS FOR EM
ROUTINE CLINICAL CARE FOR EM
VII. COMPLICATIONS VIII. REFERRAL & CO-MANAGEMENT RESOURCES IX.
A. EM CLIENT HANDOUT TEMPLATE B. ALLOPATHIC OTC OPTIONS C. COMPLEMENTARY AND ALTERNATIVE MEDICINE (CAM)
I. DEFINITIONS:
Anembryonic Pregnancy: Presence of a gestational sac without development of an embryo.
33% of early pregnancy losses are anembryonic making them the second most common reason
after chromosomal abnormalities. Previously used term = blighted ovum.
Complete miscarriage/abortion: Completed expulsion of fetal & placental tissues from the
uterine cavity. Uterus can be confirmed empty via ultrasound imaging.
Ectopic Pregnancy: About 1 in every 50 pregnancies develops outside of the uterine lining and
these are called ectopic pregnancies. Ectopic pregnancies can present with severe abdominal or
pelvic pain (usually on one side), fainting, and/or shoulder pain with or without vaginal bleeding
and they are usually not viable because they cannot continue to grow where they are implanted.
The biggest health risk with an ectopic pregnancy is rupture which can lead to internal bleeding
and be life threatening. Once an ectopic pregnancy is diagnosed, medical referral is indicated;
medical management with methotrexate may be recommended, or surgery may be necessary.
Embryonic Demise: Embryo developed, but fetal cardiac activity either did not develop
normally or stopped at some point and the pregnancy is no longer viable.
Incomplete Abortion/Miscarriage: The process of expelling the miscarriage has begun, cervix
has dilated and some of the products of conception have passed, but not all. Tissue may be
visible at cervical os or inside vaginal vault or in uterus by sonogram without evidence of viable
gestation.
Inevitable Miscarriage: Cervix has dilated and membranes may be ruptured but passage of
products has not occurred. This type of miscarriage is unavoidable and usually includes vaginal
bleeding.
Miscarriage = Spontaneous Abortion: Death of embryo or fetus before viability. This practice
guideline (PG) addresses 1st trimester miscarriage defined as up to 13 weeks + 0 days gestation.
Missed abortion: Intact gestational sac (with or without an embryo), no fetal cardiac movement,
cervix closed and may present with or without vaginal bleeding. Pregnancy determined to not be
viable, but process of expelling pregnancy has not started yet. May also be referred to as
embryonic or fetal demise, or delayed miscarriage.
Molar Pregnancy: Also referred to as gestational trophoblastic disease (GTD) or hydatidiform
mole. Molar pregnancies occur when the egg has been fertilized but instead of developing an
embryo the placenta turns into an abnormal mass of cysts as a result of a genetic error during the
fertilization process. Molar pregnancies occur in about 1 in 15,000 pregnancies in the US. In the
most serious cases of molar pregnancies the abnormal tissue can become cancerous. Therefore,
immediate medical/surgical management is indicated with quantitative human chorionic
gonadotrophin (hCG) follow up.
Products of Conception (POC): Medical term used to describe the tissue and fluids resulting
from the union of egg & sperm.
II. DIAGNOSIS OF EARLY PREGNANCY LOSS
Physiology: upon death of embryo/fetus, withdrawal of pregnancy hormones (estrogen,
progesterone, HCG) and production of other hormones (prostaglandins) help the body
detach and expel the POC. The spontaneous process may take days or weeks, producing
uterine cramping to open the cervical os and bleeding as POC is expelled. The
pathophysiology of spontaneous abortion is not well-researched.
If a woman presents with these signs/symptoms in the first trimester, miscarriage
and ectopic pregnancy should be considered and further investigation is necessary:
• Spotting/Bleeding • Passing blood clots or tissue • Abdominal pain, low back ache, menstrual like cramping, contraction like
• No fetal heart tones heard with Doppler (audio ultrasound) after 10 weeks LMP • Size/Dates discrepancy on bimanual exam • Drastic and sudden decrease in pregnancy symptoms
There are three main ways to diagnose early pregnancy loss:
1. Transvaginal ultrasound is the most common and reliable way 2. A speculum exam can be considered diagnostic if POC are visualized in the
cervical os or vaginal vault
3. A set of serial blood draws for hCG levels over several days can also determine if
a pregnancy is no longer viable if the hCG levels are dropping
III. MANAGEMENT OPTIONS FOR EARLY PREGNANCY LOSS:
• Expectant Management (EM): The process of waiting for the pregnancy to pass
on it's own without pharmaceutical medical management or uterine aspiration. EM is also referred to as "wait and see" or "the natural method". EM could possibly include the use of CAM remedies and over-the-counter (OTC) allopathic medications. EM may take days or several weeks to expel the pregnancy.
• Pharmaceutical/Medical management: Use of medications taken orally and/or
vaginally to cause the cervix to dilate and the uterus to contract in order to expel the pregnancy. The medication misoprostol (Cytotec), or a combination of misoprostol with mifepristone or methotrexate may be used in the U.S. Generally, bleeding (and likely cramping) should start within 4 hours after taking the medication if it is going to work. Sometimes more than one dose and/or more than one medication is necessary.
Note: none of the medications used for medical management of miscarriage are FDA approved for that use.
• Uterine Evacuation (sometimes referred to as surgical management):
Evacuation of retained POC with a manual vacuum aspiration (MVA) device or an electronic suction device (electronic vacuum aspiration = EVA). For first trimester pregnancy loss, uterine evacuation management can happen in an out-patient clinic or in a hospital operating room. The procedure itself only takes about 5 minutes but including intake and after care may add up to several hours at a clinic or hospital.
o Dilation & Curettage (D&C): Dilation of the cervix by a medical provider with
or without pharmaceutical assistance and scraping of the uterine lining with a curette device to remove POC. The use of an electronic suction devise, anesthesia and a paracervical block may also be included. A D&C procedure using an electronic suction device may or may not be done under ultrasound guidance. If a manual vacuum aspiration (MVA) device is used for a D&C ultrasound could be used but is not mandatory. The term D&C is used loosely and also may include MVA.
o Manual vacuum aspiration (MVA): Use of non-electrical suction with a MVA
device that has a plastic suction tube. This procedure can happen quickly (5 minutes) in an out-patient clinic. Usually involves oral pain medication, a paracervical block and sometimes light IV sedation. The MVA suction syringe is used for gestations up to 12 weeks 6 days determined by last menstrual period (LMP). There is debate on whether a MVA is considered a surgical procedure because no surgical equipment is necessary and using an MVA for miscarriage management is within the scope of practice for providers who do not perform surgical procedures such as: Family medicine physicians (MD, DO), Advanced Nurse Practitioners (ARNP), Certified Nurse Midwives (CNM), and Physician Assistants (PA).
IV. CANDIDACY & CONTRAINDICATIONS FOR EM
Good Candidates for EM:
Women who have a confirmed first
Not currently bleeding heavily
trimester nonviable intrauterine pregnancy No fever
No signs of infection
No abnormal smelling discharge
Client expresses desire for EM
Competent enough to monitor own
Competent enough to monitor blood loss
temperature
Sur & Raine-Fenning, 2009
*Further considerations may include: access to 24-hour transportation to a hospital if
needed and living in close range of a hospital with 24-hour care in case complications
arise and emergency surgical evacuation is indicated.
Contraindications for EM:
Uncertain diagnosis
Severe pain uncontrolled by OTC
Signs of infection: fever, chills, uterine
tenderness, abnormal smelling discharge or blood
Diagnosed molar pregnancy
Ectopic pregnancy
Miscarriage of unknown location
Suspected gestational trophoplastic disease
(pregnancy not seen in ultrasound inside
(hydatidiform mole or "molar" pregnancy)
uterus) Indicated karyotyping or histological
Gestation beyond 13 weeks
diagnosis Twin pregnancy (*EM may be okay if only History of anemia or coagulopathies one fetus has passed and the other is still viable) El-Sayed et al., 2009 and Oliver & Overton, 2014
Note: Choosing EM is a personal choice and therefore shared decision making is essential. Each woman experiences miscarriage in her own way, influenced by her culture, personal history, the meaning of the pregnancy to her, and so forth. Although she may be a good candidate for EM based on meeting criteria for the indications and contraindications listed above, a woman's lack of interest in trying EM is a contraindication to this management option. Women should be reassured that all of the miscarriage management options are safe and that the choice of treatment will not affect her future fertility.
V. PROS AND CONS OF EM
Pros of EM:
As long as there is no hemorrhage, fever or infection, there is no time limit to how long it
is safe to wait for a miscarriage to occur naturally
Inexpensive
Non-invasive. Avoidance of anesthesia & surgical risks
Some women feel this option gives them more control of the situation
There is always the option to seek medical management, uterine aspiration or D&C if
desired
High success rate (most successful in the case of incomplete miscarriage)
Low complications rate
El-Sayed, Mohamed & Jones, 2009; Prine & Macnaughton, 2011; Sur & Raine-Fenning, 2009
Potential Cons of EM:
It may take weeks to complete the passage of the tissues
May experience ongoing heavy bleeding and cramping
Passage of the products of conception, bleeding and cramping is unpredictable
Follow up appointment is important to assess completion of miscarriage
The emotional toll of prolonging the completion of a miscarriage can be significant
Possibility of infection developing while waiting for completion of miscarriage
El-Sayed, Mohamed & Jones, 2009; Sur & Raine-Fenning, 2009
VI. ROUTINE CLINICAL CARE for EM The basics of EM are:
• Anticipatory Guidance: Midwife explains what to expect with the client:
o Pain related to a miscarriage can be as severe as labor, but subsides
quickly once POC has passed
o Review of warning signs/symptoms that they should inform the midwife
o The woman can go about her daily life, letting her body take care of
expelling the pregnancy
• The midwife must make himself or herself available for support during and for
some time after the process.
• Emotional support is important - the midwife should recognize when referral is
necessary for psychological and emotional issues that are beyond their skill and scope to manage independently.
• It is essential that ectopic and molar pregnancies be ruled out before starting
expectant management, as these types of pregnancies need immediate referral for special care. Note: The management options for each kind of intrauterine spontaneous abortion
are the same. However, the success rate with EM often depends on the type of miscarriage a woman is experiencing.
Incomplete/inevitable miscarriage
91% complete with EM only
Embryonic demise
76% complete with EM only
Anembryonic pregnancy
66% complete with EM only
EM Clinical Care
Pre-expulsion Phase
• How long is too long for EM? Much of the research followed the ‘2-week rule',
but in the absence of complications, and a desire by the woman to continue expectant management there is no time limit to waiting for the body to naturally expel a spontaneous first trimester miscarriage.
o If the process of expelling the POC has not started by 8 weeks after
diagnosis of a non-viable pregnancy then the client & midwife should review management options again. If menstrual periods have resumed, the miscarriage can be considered complete. If there is any question or confusion about this, an ultrasound could confirm completion.
Frequency of contact:
§ During the pre-expulsion phase an initial visit in person to review options, offer
emotional support, and agree upon a plan is suggested. Client & midwife will decide if an in person visit is necessary. Phone discussion may be adequate.
§ Give or email the client who chooses EM a handout that clearly outlines what to
expect, warning signs/symptoms and instructions on when to contact midwife. (see Appendix A)
§ Obtain labs for Hct/Hgb and blood type if not already documented in the client's
§ Discuss CAM therapies if the client is interested. (see Appendix C) § Encourage clients to tell someone in their life what they are going through and
check in with them about emotional support.
§ Offer weekly phone calls to check in on the client's emotional well-being as well
as reviewing her physical symptoms.
Rh(D) immune globulin (RhIG) (50 mcg dose for <12 wks) should be given to Rh
Negative (Rh-) women within 72 hours of the first incidence of bleeding after an informed consent discussion. If it is not given in this time, it should still be offered. If the 50 mcg dose is unavailable, the standard more available 300 mcg dose is also appropriate (ACOG, 2015). Note: Although there is no strong evidence to support the need for RhIG in early pregnancy loss, it remains the standard of care in the US.
During Expulsion
§ Advise woman to notify midwife once the cramping & bleeding begins. § Remind the woman to take her temperature every 4 hours (or more often if she
feels feverish) during the expulsion process.
§ Explain the difference between normal bleeding and excessive bleeding; remind
the client to refer to the handout she was given.
§ Acknowledge that she will likely experience pain and can use OTC pain
medication and CAM options as needed. (see Appendix B)
§ Strongly encourage her to not be alone during expulsion. § Once expulsion process is complete remind the woman to take her temperature
twice daily or more often if she feels feverish.
Post-Expulsion Phase
§ Optional in person visit once expulsion process is complete. Evaluate well-being:
blood pressure, temperature, pulse, amount of bleeding, emotional status, support system evaluation, review of danger signs.
§ If the client is Rh- and has not yet gotten RhIG, administer ideally within 72 hours
after first incidence of bleeding.
§ Discuss the option of getting an ultrasound to confirm expulsion is complete –
this is considered based on the clinical picture and the client's preferences.
§ Recommend "pelvic rest" - no vaginal sexual activity or tampons for 2 weeks. § It may be difficult for a woman to return to the clinic where she had her prenatal
care especially if she is likely to see other pregnant women and new babies while waiting. Depending on the situation a home visit may be appropriate.
Follow-Up Contacts
Optional weekly phone calls to discuss:
§ Physical symptoms § Support system § Emotional well-being § Answer questions
Optional final post miscarriage in-person follow up care (usually 2 weeks post-
expulsion) may include, depending on the clinical picture:
§ Ultrasonography to confirm uterus is empty if indicated – persistence of
pregnancy symptoms, ongoing vaginal bleeding/spotting, client need for reassurance.
§ Lab work to confirm an 80% drop in the b-HCG levels – this should occur by one
week following complete passage of tissues. By 6 weeks post expulsion b-HCG levels should be negligible or absent.
§ Lab work for Hgb, Hct, or CBC to evaluate for anemia and suggest supplements if
§ Emotional support to process the experience, including the co-parent if indicated* § Altered grieving and depression evaluation to determine if a counseling referral
may be appropriate.
§ Contraception/Family Planning per the client's preference. § Anticipatory guidance for attempting pregnancy in the future, per the client's
*Recommendations for rituals after loss: It may be a good idea to encourage clients to have a ceremony and light a candle for the baby that they lost. Other suggestions are to write a letter to the baby, make artwork, get a memorial piercing or tattoo, plant a tree or special flower in the baby's memory. It may be helpful for the midwife to address that grief may return around the time of the estimated due date and/or if she experiences another pregnancy in the future. Remember to be culturally sensitive while discussing grief & loss.
This is also a good opportunity for the midwife to point out the wisdom and amazing capacity of the human body because it knows when and how to end a nonviable pregnancy. An estimated 30% of all pregnancies end in miscarriage and 50% of those are due to chromosomal abnormalities. Helping the person experiencing pregnancy loss put some trust in their body that it did exactly what it was supposed to do (even if we don't get to know the reasons why) may help with the healing process.
VII. COMPLICATIONS
Consultation &/or referral is indicated:
Severe or prolonged emotional distress, depression, or grief reactions Infection:
• Fever (>100.4 F) • Uterine tenderness • Foul smelling discharge or blood
Hemorrhage (soaking more than 2 menstrual pads in 1 hour, or passing several clots larger than a golf ball) Severe pain anywhere Extreme pain not controlled by OTC pain medications
Signs/symptoms the midwife & client should watch for*
Excessive bleeding (soaking more than 2 menstrual pads in 1 hour or actively bleeding with a steady stream) Infection (any of the following):
• Fever (>100.4 F) • Tender uterus (possible endometritis) • Foul smelling discharge or blood
*If these complications arise immediate uterine aspiration is recommended.
• Gynecological infection rates related to miscarriage are rare (2-3% overall) no
matter what type of management is used. Midwife & client must monitor for signs of infection (listed above) and seek uterine aspiration options if these signs arise.
• Hemorrhage associated with EM is rare, but the midwife needs to counsel and
monitor for this complication.
o a steady stream of blood loss or soaking 2 menstrual pads in 1 hour might
require a call to emergency medical services.
• Severe or prolonged emotional distress is one reason that women decide to change
their management route from EM to a quicker option. Help clients understand that once EM is chosen they have the option to change management plans with full support from their midwife.
Spectrum of expected and potentially complicated grief reactions:
Normal grief responses (usually
Complicated grief reactions (consistent,
temporary):
disruptive, pervasive, long-lasting):
Retreating from social activities
Feelings of guilt and self-blame
Intrusive thoughts that subside with time
Feelings of yearning for what they lost
Feeling like their body failed them
Numbness that subsides with time
Feelings that their femininity has been sabotaged
Impairment of day-to-day functioning
Major changes in eating, sleeping, hygiene, self-care
Kersting & Wagner, 2012 *Note: grief and loss experiences and expressions vary depending on culture, religion, family, and personal history. Evaluation and care must be individualized.
VIII. REFERRAL & CO-MANAGEMENT RESOURCES
Referral options for physical care:
§ Medical physicians (MD, DO): gynecologists, obstetricians, or family physicians
with uterine evacuation capabilities
§ Advanced practice clinicians (CNM, ARNP, PA, NP, CRNA): may or may not
have uterine evacuation capabilities, so find out services provided before referral
§ Hospital emergency department: should have an obstetric provider on call. § Naturopathic doctor (ND): may or may not have uterine evacuation capabilities,
but can support the miscarriage process with professional evaluation and treatment with naturopathic treatments
§ Traditional Chinese Medicine (TCM) practitioner: acupuncturist or herbalist to
support the miscarriage process
Referral sources for emotional / mental health care:
• Psychotherapists • Psychologists • Psychiatrists (can prescribe medications) • Spiritual counselors • Full spectrum doulas with experience in miscarriage • Physicians or advanced practice clinicians with counseling skills (can prescribe
• NDs (can prescribe medications and CAM remedies) • Acupuncturists
Internet support:
· http://nationalshare.org/
· http://www.miscarriagesupport.org.nz/
· http://stillstandingmag.com/
· http://www.stillbirthday.com/
IX. REFERENCES Allison, J. L., Sherwood, R. S., & Schust, D. J. (2011). Management of first trimester pregnancy loss can
be safely moved into the office. Reviews in Obstetrics & Gynecology, 4(1), 5-13. doi:10.3909/riog0142
American College of Obstetricians & Gynecologists (ACOG). (2012). Dilation & Curettage Frequently
Asked Questions FAQ062 Special Procedures. Retrieved from: https://www.acog.org/ /media/For%20Patients/faq062.pdf?dmc=1&ts=20140922T1301355547
American College of Obstetricians and Gynecologists (ACOG). (2015). Practice Bulletin Clinical
Management Guidelines for Obstetrician-Gynecologists #150: Early Pregnancy Loss. The American College of Obstetricians and Gynecologists Women's Health Care Physicians, 125(5), 1258-1267.
Cappiello, J. (n.d.) Advancing scope of practice in reproductive care. [PowerPoint slides]. Retrieved from:
Dangalla, D. P. R., & Goonewardene, I. M. R. (2012). Surgical treatment versus expectant care in the
management of incomplete miscarriage: A randomised controlled trial. Ceylon Medical Journal, 57, 140-145.
Darney, B. G. (n.d.) MM-TI Miscarriage management-training initiative. Retrieved from:
El-Sayed, M. M., Mohamed, S. A., & Jones, M. H. (2009). Expectant management of first-trimester
miscarriage. Journal of Obstetrics and Gynaecology, 29(8), 681-685.
Fritz, S. (2012). Essential Oils for Pregnancy, Birth & Babies. Sierra Vista, Arizona: Gently Born
Geraghty, B. (1997). Homeopathy for Midwives. New York: Churchill Livingstone.
Godfrey, E. M., Leeman, L., & Lossy, P. (2009). Early pregnancy loss needn't require a trip to the
hospital. The Journal of Family Practice, 58(11), 585-590.
Goldberg, A. B., Carusi, D., & Westhoff, C. (2009). Chapter 17: Pregnancy loss. In Paul, M., Lichtenbert,
E. S., Borgatta, L., et al. (Eds.), Management of Unintended and Abnormal Pregnancy: Comprehensive Abortion Care (1st ed.), (pp. 264-279). Chichester, W. Surry, UK: Wiley-Blackwell.
Kersting, A., & Wagner, B. (2012). Complicated grief after perinatal loss. Dialogues in Clinical
Neuroscience, 14(2), 187-194.
King, T. L., Brucker, M. C., Kriebs, J. M., Fahey, J. O., Gegor, C. L., & Varney, H. (2015). Varney's
Midwifery, (5th ed.). Burlington, MA: Jones & Bartlett Learning.
Oliver, A., & Overton, C. (2014). Diagnosis and management of miscarriage. The Practitioner, 258(1771),
Prager, S. (2013). Do nothing, do something, do surgery: Management of early pregnancy loss.
Prine, L. W., & Macnaughton, H. (2011). Office management of early pregnancy loss. American Family
Physician, 84(1), 75-82.
Ridiman, K. M. (1997). Supporting a mother whose pregnancy has ended. Midwifery Today, 41, 26-28.
Romm, A. (2010). Botanical Medicine for Women's Health. St. Louis, MO: Churchill Livingstone
Sur, S. D., & Raine-Fenning, N. J. (2009). The management of miscarriage. Best Practice & Research
Clinical Obstetrics and Gynaecology, 23, 479-491.
Tulandi, T., & Al-Fozan, H. M. (2014). Spontaneous abortion: Management. UpToDate. Retrieved from:
Tulandi, T., & Al-Fozan, H. M. (2014). Spontaneous abortion: Risk factors, etiology, clinical
Trinder, J., Brocklehurst, P., Porter, R., Read, M., Vyas, S., & Smith, L. (2006). Management of
miscarriage: Expectant, medical, or surgical? Results of randomised controlled trial (miscarriage treatment (MIST) trial). BMJ, 332(1235), 1-6. Retrieved from: http://www.bmj.com/content/332/7552/1235
Weed, S. (1986). Wise Woman Herbal for the Childbearing Year. Woodstock, NY: Ash Tree Publishing. World Health Organization (WHO). (2003). Safe abortion: Technical and policy guidelines for health
systems. Geneva: WHO. Retrieved from: http://whqlibdoc.who.int/publications/2003/9241590343.pdf
APPENDIX A: Sample Client Handout
(Practice name & contact info)
Expectant Management of First Trimester Miscarriage
Expectant management of miscarriage is the process of waiting for a non-viable pregnancy to pass on it's own without pharmaceutical (medication) or uterine aspiration methods of removal. It's normal for expectant management to take several days or weeks for the miscarriage to be completed.
What to expect:
1. Once the active phase of the miscarriage starts you will experience strong
menstrual like cramping (some compare it to labor contractions) and bleeding. These cramps could be intense for a few hours while the body is expelling the pregnancy, but afterwards they should subside.
1. Bleeding will likely be similar to a heavy menstrual period. Passing a few blood
clots (smaller than a golf ball) & tissue is normal. Bleeding can last 2-4 weeks after the miscarriage is complete.
2. Once the cramping & bleeding starts you should monitor your temperature every
4 hours and report any readings >100.4 F (or 38 C) to your midwife.
3. Be sure to practice good self-care during this process and pay attention to getting
enough to eat & drink, and also you need your sleep.
4. If your blood type is Rh Negative, you can discuss with your midwife if you
should get a "RhoGAM" injection.
5. Once the miscarriage is complete it is advised to avoid tampons, douching and
vaginal sexual activity for 2 weeks to reduce the chance of infection.
6. Before starting sexual relations, talk to your midwife about birth control
(contraception) or, if you want to get pregnant again right away, how to decide when you and your body are ready.
REASONS TO CALL YOUR MIDWIFE IMMEDIATELY, DAY OR NIGHT:
Excessive bleeding may include:
• Soaking 2 menstrual pads in 1 hour • Actively bleeding with a steady stream • Passing several blood clots the size of a golf ball or larger
Fever (>100.4 F or 38 C) Extreme pain uncontrolled by over-the-counter pain medications Uterus feels tender, sore or you are experiencing sharp pains in your abdomen Foul (bad) smelling discharge or blood
Pain management:
Ibuprofen (Advil, Motrin)
800 mg first dose, then 600 mg every 6 hours until
*this type of medication is most effective for
miscarriage is complete. Do not exceed 2400 mg in 24
uterine cramping
hours. Take with food.
Naprosyn/Naproxen/
500 mg (Naproxen) or 550 mg (Naproxen Sodium) every
Naproxen Sodium (Aleve)
12 hours. Do not exceed 1250 mg in 24 hours. Take with
* this type of medication is most effective for
uterine cramping *Take one or the other; do not use both at the same time
Pain management:
Acetaminophen (Tylenol)
650-1000 mg every 4-6 hours. Do not exceed 3000 mg in
*may use if allergic to Ibuprofen or Naprosyn, 24 hours. but does not work as well as those medications for this type of pain Cramp Bark tincture
Take as directed on bottle.
What if I change my mind? Once expectant management is started you have the option to
change management plans if you desire. If complications arise during expectant management
uterine evacuation methods will likely be necessary. Your midwife will refer you to an advanced
practice clinician that can help you. Please note that the medical term for "miscarriage" is
"spontaneous abortion" or "SAB" – you might hear the nurses and doctors use this phrase when
they talk to you. Here are your other options and what to expect:
• Pharmaceutical/Medical management: Use of prescription medications taken orally
and/or vaginally to cause the cervix to dilate and the uterus to contract in order to expel the pregnancy. The medication misoprostol (Cytotec), or a combination of misoprostol with mifepristone or methotrexate may be used. This process can take hours to a couple of days to completely pass the pregnancy. You may need more than one dose of the medication/s.
• Uterine Evacuation (sometimes referred to as surgical management or D&C):
Evacuation of the pregnancy with a manual vacuum aspiration (MVA) device or an electronic suction device. Evacuation may or may not include pharmaceutical anesthesia sedation and/or numbing medications injected into the cervix. For first trimester pregnancy loss, uterine evacuation management can happen in an outpatient clinic or in a hospital. The procedure itself only takes about 5 minutes but including intake and after care may add up to several hours at a clinic or hospital.
Emotional Care
It is important that you pay attention to the emotional reactions you have to the loss of
your pregnancy. It is normal to grieve and feel sad, and every person will have a unique experience. One person's reaction can be really different from another person's reaction, and there is a wide range of normal experiences. Your midwife wants to support you, and people in your life who are close to you may also be valuable resources for you. Some people find information and community online; a few websites are referred to below. If you or your friends/family think your emotional reaction is severe, or going on for a long time, your midwife might recommend that you see a professional counselor or spiritual advisor. Internet support: · http://nationalshare.org/ · http://www.miscarriageassociation.org.uk/support/ · http://www.miscarriagesupport.org.nz/ · http://stillstandingmag.com/ · http://www.stillbirthday.com/
APPENDIX B
Allopathic OTC Medications
Pain Management:
Ibuprofen (Advil, Motrin)
800 mg first dose, then 600 mg every 6 hours until
*works best on uterine receptors
miscarriage is complete. Do not exceed 2400 mg in 24 hours. Take with food.
Naprosyn/Naproxen/Naproxen 500 mg (Naproxen) or 550 mg (Naproxen Sodium) Sodium (Aleve)
every 12 hours. Do not exceed 1250 mg in 24 hours.
*works best on uterine receptors
*Take one or the other; not both at the same time Acetaminophen (Tylenol)
650-1000 mg every 4-6 hours. Do not exceed 3250 mg
*may use if allergic to Ibuprofen
or Naprosyn, but does not work as
well as those medications for this
type of pain
Epocrates. (2015)
Sleep Medications to help with insomnia caused by anxiety or stress (see also CAM
options):
diphenhydramine (Benedryl)
Take 25-50 mg 30 minutes before bed and if needed every 4-6 hours at night. Do not exceed 300 mg in 24 hours.
doxylamine (Unisom)
Take 25-50 mg 30 minutes before bed and if needed every 4-6 hours at night.
CAM Support
INDICATION & RECOMMENDATION
Promote expulsion:
Black & Blue Cohosh
20 drops of each black & blue cohosh tincture every
hour to promote uterine contractions & empty the uterus. Do not exceed 5 doses.
Clary sage essential oil Apply & massage drops of clary sage topically to lower
abdomen to promote uterine contractions and assist in passing remaining tissue.
Evening Primrose Oil
Two 500 mg capsules taken orally twice daily for 2 days Aviva Romm
& 1500 mg vaginally to help ripen cervix.
Mixture of Cotton root After 24 hours of EPO (listed above) start taking
bark, black cohosh &
tincture mixture of: 40 mL cotton root bark, 40 mL
black cohosh and 20 mL of blue cohosh for a total of 100 mL. Take 2.5 mL of this mixture orally every hour for 4 hours and then discontinue. If no contractions occur try again next day. If again no contractions occur do nothing on day 3. Try same dose of tincture mixture on day 4 and 5 if needed.
Cramp Bark tincture
Take as directed on the bottle for pain caused by uterine
RESCUE Remedy flower essence is made up of 5
individual flower remedies that help during the
emotional impact of a stressful situation. 1) Rock
rose is used for terror and panic. 2)
Impatiens addresses irritation and impatience. 3)
Clematis is for inattentiveness and a lack of focus. 4)
Star of Bethlehem is for shock. 5) Cherry plum helps
with irrational thoughts and a lack of self control. Take
as indicated on bottle.
Good for patients with irritability, insomnia, and
anxiety. It can also be used for pain, inflammation, infection, as a general tonic to improve mental state, and can give energy for patients experiencing stress-induced illness or exhaustion. Ashwagandha has a calming effect on the nervous system and it is reported to be a hematopoietic, making it useful in the treatment of anemia. Take as indicated on bottle.
Used for the treatment of fatigue, depression, anemia,
GI ailments, infections, nervous system disorders and to promote physical endurance, longevity and work productivity. Take as indicated on bottle.
INDICATION & RECOMMENDATION
Bleeding:
Shepherd's purse
10-20 drops under tongue to control excess bleeding as
often as needed. *Client should always consult with the midwife before independently undertaking herbal treatments for excessive bleeding.
Witch hazel bark
10-20 drops under tongue to control excess bleeding as
often as needed. *Client should always consult with the midwife before independently undertaking herbal treatments for excessive bleeding.
Sleep aid. Take 1-5 mg before bed.
Used to temporarily relieve the symptoms of simple
nervous tension, restless sleep, and occasional
sleeplessness. Take as indicated on bottle.
fort%C3%A9%C2%AE
Herbs for Sleep Promotion
Therapeutic Activity
California Poppy
Tranquilizer & Sedative & Hypnotic
Tranquilizer & Sedative
Tranquilizer & Anxiolytic
Tranquilizer & Sedative
Tranquilizer & Sedative
Tranquilizer & Sedative & Anxiolytic
Tranquilizer & Sedative & Anxiolytic
Sedative & Hypnotic & Anxiolytic
Sedative & Anxiolytic
Sedative & Hypnotic & Anxiolytic
Adapted from Romm, 2010, p. 491 Emmenagogues are herbs that can stimulate menstruation. They are sometimes referred to as abortifacients but there are many reasons that emmenagogues are used that are not related to inducing abortion. An inexperienced LM should consult, co-manage or refer out clients that desire the use of these herbs.
There are several websites online that explain herbal emmenagogues. The LM
must be alert for bias and agenda-driven rhetoric while reading because some have an anti abortion agenda.
Homeopathy
Generally/Emotionally:
Anxiety, restlessness,
fear of death or something bad happening
Not specific to Profuse,
"Stinging pain in
Fear of being alone.
Tearful & whining.
becoming more and more frequent until uterine contractions are produced. The flow then begins. Labour-like in uterine region extending to thighs (Geraghty, 1997, p. 51)"
"Sore and bruised
(Geraghty, 1997, p.
Caulophyllum Not specific to Scanty,
Possible history of
spontaneous abortion,
spasmodic bearing
fear, irritability,
down, cramping in
the abdomen centred low down in the pelvis, severe and tormenting back pain (Geraghty, 1997, p. 51)"
"Pain predominates
Mild, weepy, apologetic.
May want plenty of
alternates with the
company to offer their
pains (Geraghty,
support and sympathy.
when it starts again, black or bright red clots
Table adapted from: Geraghty, 1997, p. 51-52
Source: http://www.washingtonmidwives.org/documents/conferenceslides/cardinal-raelene-loss-miscarriage.pdf
This article was published in an Elsevier journal. The attached copy is furnished to the author for non-commercial research and education use, including for instruction at the author's institution, sharing with colleagues and providing to institution administration. Other uses, including reproduction and distribution, or selling or
SRAC Publication No. 473 Southern regional Medicated Feed for Food Fish Anita M. Kelly1 Medicated feed is frequently recommended to control drugs for use in aquaculture, preventing bacterial disease bacterial disease outbreaks in cultured fish. Medicated outbreaks with proper disease management strategies is feeds are commercially prepared, and contain an anti-







