Gbhs.on.ca
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Grey Bruce Health Services
Pandemic Influenza Plan
Chapter 1 – Introduction
Chapter 2 - Incident Management System (IMS)
Chapter 3 - Ethical Framework
Chapter 4 – Infection Control
Infection Prevention and Control Program Pandemic Plan…………
Chapter 5 - Capacity Assessment, Triage and Bed Management Emergency Department…….…………………………………………
Women & Child Care .…………………………………………………… 34 Surgical & Ambulatory Care.………………………………………….
Rehabilitation & Restorative Care .……………………………………
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Chapter 6 - Laboratory/Diagnostic Imaging Services
Chapter 7 - Pharmacy
Chapter 8 - Human Resources
Chapter 9 - Material Management and Logistical Services
Material Management …………………………………………………… 79
Chapter 10 – Information Technology
Chapter 11 - Security, Parking and Transportation
Security, Parking and Transportation Services……………………… 86
Chapter 12 - Plant Operation, Maintenance and Environmental
Services
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Chapter 13 – Visitors
Chapter 14 - Communications, Education, Stakeholder
Relations and Public Relations………………………………….…
Chapter 15 – Post-Pandemic Period
Chapter 16 - Appendix
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
PANDEMIC INFLUENZA RESPONSE (CONTINGENCY) PLAN
CHAPTER 1: INTRODUCTION
Influenza (flu) has been with us for centuries. This respiratory disease causes severe
illness and death each winter in Canada.
"During the 20th century, influenza pandemics caused millions of deaths, social
disruption and profound economic losses worldwide. Influenza experts agree that
another pandemic is likely to happen but are unable to say when. The specific
characteristics of a future pandemic virus cannot be predicted. Nobody knows how
pathogenic a new virus would be, and which age groups it would affect. The impact of
improved nutrition and health care needs to be weighed against the effect of increased
international travel or simultaneous health threats that weaken the immune system
. The
level of preparedness will also influence the final death toll. However, even in one of the
more conservative scenarios, it has been calculated that the world will face up to 233
million outpatient visits, 52 million hospital admissions and 7.4 million deaths globally,
within a very short period of time". (WHO Influenza Checklist 2005)
Goals of the GBHS Pandemic Plan
To protect patients and staff and to minimize serious illness and death
To minimize the psychological, social and economic impact of the illness
To minimize disruption in the facilities and allow for ongoing day-to-day operations,
To develop a strategic approach to a possible pandemic in cooperation with the Grey
Bruce Health Unit and our partner health care providers across Grey & Bruce counties.
To identify and discuss all ethical considerations (i.e. lack of human resources,
supplies, and equipment , antivirals, vaccines, ventilators and beds)
Key Planning Assumptions:
A pandemic will likely be due to a new subtype of influenza A that we will have no
immunity to, however the incubation period, period of communicability and method of transmission for the novel strain are assumed to be consistent with other known influenza strains.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
It is unlikely that an effective vaccine will be available at the start of pandemic
influenza activity in Canada. An effective vaccine may be available for a second wave of the pandemic.
A new strain is most likely respiratory and likely originate in Southeast Asia New subtype of influenza A will develop outside Ontario but arrive with little lead time
after declaration by the WHO.
Pandemic influenza usually spreads in two or more waves, ether in the same year or
in successive influenza seasons (i.e. October to April). A second wave may occur within three to nine months of the initial outbreak wave and may cause more serious illnesses and deaths than the first. In any locality, the length of each wave of illness is approximately six to eight weeks. As a pandemic wave passes through a community, it is likely that most cases of influenza will be caused by the pandemic strain (Prevention and Control of Influenza during a Pandemic for All Healthcare Settings; Annex F, May 2011).
The incubation period for influenza is from 1-3 days. People with influenza are infectious and able to transmit the virus for up to 24 to 48
hours before onset of symptoms and for up to 7 days after (i.e. for 3-5 days from onset in adults and up to 7 days in children).
The influenza virus is highly contagious, spread by people coughing or sneezing into
the air, or by touching contaminated environmental surfaces.
The virus can survive on unwashed hands for 5 minutes, on tissues or clothing for 8
to 12 hours and on hard surfaces such as tables or telephones for 24 to 48 hours.
It is anticipated that upwards of 35% of healthcare workers will miss work either from
illness or caring for family members throughout the pandemic. At the peak of the pandemic, 20 – 25% of the workforce may be absent.
Of those patients who become ill, 55% will require medical care – of whom 53% will
require outpatient or primary care and 1.5 – 2% will require hospitalization.
Individuals who recover from infection caused by the pandemic influenza strain
should be immune to further infection from that specific strain.
Within Grey and Bruce Counties, this means that we should expect:
30,013 outpatient visits
871 hospitalizations
184 fatalities
Vaccines will be allocated to the GBHU & distributed to GBHS based on our
identified numbers of health care workers.
Antivirals will be distributed through community pharmacies.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Shortage of antivirals will cause people to panic whether it be Health Care
Professionals or the Community at large.
Vaccine when available will be for only a certain sector of people (as determined by
the MOH) – raising anxiety for the community at large.
During an Influenza Pandemic, Health Care Settings will need large quantities of
equipment and supplies to provide care & to protect health care workers.
Demand will be high worldwide, and traditional supply chains may break down. Being in a rural area – it may be harder to get supplies There will be misconceptions or speculations about what is happening internally and
externally (in the community and the world).
Communications will play a huge role in disseminating directives and other material
from the Ministry of Health and Long-Term Care and the Grey Bruce Health Unit.
Need timely and accurate messages and information re: the Pandemic and what is
happening within GBHS.
Clinical Assumptions:
Maintain business until Pandemic reaches Grey Bruce
Ambulatory non-urgent clinics will be cancelled
All elective surgeries, if they do not affect the patient's short term outcome, will be cancelled.
Even though some elective procedures will be cancelled – the Health Care Facilities will be full with ill patients – supplies will still be needed throughout this influenza Pandemic Period.
"Life or Limb" interventions will occur
Rural site OR's will be closed
Public Health will not have "Flu Centers" so the hospitals will become the center by default
We will be able to provide a minimum of security for our screening center and /or access to hospital
Dialysis will continue to operate
Oncology will continue to operate with certain reductions
We will be working in partnership with our partner organizations Hanover District Hospital and South Bruce Grey Health Center to continue to provide services across our counties. This may result in redistribution of services, supplies and staff.
Funeral homes/transportation for bodies available
Nursing homes will take care of their patient for as long as possible.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Regardless of which unit/program /service is cancelled, no staff members will be cancelled. All available staff members will be redeployed as needed.
We will have a greater volume in our catchment area related to cottagers settling in their summer residence to avoid the cities.
All patients and staff will be wearing a mask. It is assumed that everyone is contagious during the entire phase 6 of the pandemic.
Primary HR issue will be to maintain adequate staffing levels to manage the existing and additional workflow resulting from the pandemic event.
With the influx of new patients ill with the influenza, in addition to the regular work demands, adequate staffing will not be available and decisions will have to be made regarding work priorities.
Communication/Education Assumptions
1. Obtaining and sharing timely and accurate information will be one of the most
important facets of the pandemic response
2. Consistency of messages across all sectors and levels is essential
3. Messages will change over the duration of the pandemic, as additional
information about the virus, burden of the disease and management strategies are understood
4. There will be a large demand for information on circulation of a pandemic
strain, symptoms of the disease, burden of the disease, access to care, steps for self care, up-to-date information on PPE, status of services, availability of antivirals and vaccines
5. Potential for misunderstanding and skepticism about information exists given
the challenge of clear direction from the province during the SARS experience
Planning Stages
The World Health Organization has created a number of phases to describe the stage at
which a pandemic exists. These common definitions facilitate clear communication
about the level of risk that is being described. These phases were revised in 2009.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Table 1: WHO Pandemic periods and Phases (source: World Health Organization,
2005)
Interpandemic Period
No viruses circulating among animals have been reported to cause infections in humans.
An animal influenza virus circulating among domesticated or wild animals is known to have caused infection in humans, and is therefore considered a potential pandemic threat.
Pandemic Alert period
An animal or human-animal influenza reassortant virus has caused sporadic cases or small clusters of disease in people, but has not resulted in human-to-human transmission sufficient to sustain community-level outbreaks. Limited human-to-human transmission may occur under some circumstances, for example, when there is close contact between an infected person and an unprotected caregiver. However, limited transmission under such restricted circumstances does not indicate that the virus has gained the level of transmissibility among humans necessary to cause a pandemic.
Is characterized by verified human-to-human transmission of an animal or human-animal influenza reassortant virus able to cause "community-level outbreaks." The ability to cause sustained disease outbreaks in a community marks a significant upwards shift in the risk for a pandemic. Any country that suspects or has verified such an event should urgently consult with WHO so that the situation can be jointly assessed and a decision made by the affected country if implementation of a rapid pandemic containment operation is warranted. Phase 4 indicates a significant increase in risk of a pandemic but does not necessarily mean that a pandemic is a forgone conclusion.
Is characterized by human-to-human spread of the virus into at least two countries in one WHO region. While most countries
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
will not be affected at this stage, the declaration of Phase 5 is a strong signal that a pandemic is imminent and that the time to finalize the organization, communication, and implementation of the planned mitigation measures is short.
Pandemic period
The pandemic phase, is characterized by community level
outbreaks in at least one other country in a different WHO
region in addition to the criteria defined in
Phase 5.
Designation of this phase will indicate that a global pandemic
is under way.
Post Peak Period
Pandemic disease levels in most countries with adequate surveillance will have dropped below peak observed levels. The post-peak period signifies that pandemic activity appears to be decreasing; however, it is uncertain if additional waves will occur and countries will need to be prepared for a second wave.
Previous pandemics have been characterized by waves of activity spread over months. Once the level of disease activity drops, a critical communications task will be to balance this information with the possibility of another wave. Pandemic waves can be separated by months and an immediate "at-ease" signal may be premature.
Post pandemic period
Influenza disease activity will have returned to levels normally seen for seasonal influenza. It is expected that the pandemic virus will behave as a seasonal influenza A virus. At this stage, it is important to maintain surveillance and update pandemic preparedness and response plans accordingly. An intensive phase of recovery and evaluation may be required.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
The WHO phase number reflects the international risk or activity level with respect to the
new influenza virus subtype but may not reflect virus activity in Canada especially during
the pandemic alert period. The Public Health agency of Canada has developed a
numbering system to reflect pandemic influenza activity in Canada:
WHO Phase
Definition
Outside Canada increased and sustained transmission in the general population has been observed. No cases have been detected in Canada.
Single human case(s) with the pandemic virus detected in Canada. No cluster(s) identified in Canada.
Localized or widespread pandemic activity observed in the Canadian population.
Roles and Responsibilities of Pandemic Planning (Source: Ontario Health Pandemic
Influenza Plan)
Municipal government and local public health authorities are responsible for
coordinating local response to influenza pandemic, including:
Maintaining a local surveillance system, reporting clusters of FRI (Febrile Respiratory
Illness), ILI (Influenza Like Illness), and investigating outbreaks
Developing plans to provide mass immunization and distribute vaccines and antiviral
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Liaising with local partners(e.g. emergency responders, hospitals, community
services, mortuary services, schools, workplaces)
Assessing the capacity of local health services, including health human resources,
and identifying additional /alternative resources.
Defining clear responsibilities for communication at the local and facility level during
Collaborating with the provincial government to deliver public information/education
Strategic Approach:
Be ready – develop a plan for the Grey Bruce Health Services in cooperation with the
Health Unit and community and regional partners.
Be Watchful- institute active screening and upgrade as the pandemic develops and
provide surveillance activities to identify the earliest signs of a pandemic
Be decisive – manage the spread quickly and effectively
Be transparent – communicate with stakeholders, the staff and the public early in the
process and update, as information becomes available.
Be Ready:
To be ready implies that the organization has early systems in place to screen
and provide surveillance to contain the spread and minimize the overall impact of the pandemic.
Active screening (for Febrile Respiratory illness) is being done:
In the Emergency Departments
Same day admit
Pre Surgical Screening
Day
Oncology Dialysis Occupational Health & Safety
A computerized
screening form is now being used in Firstnet, surginet and carenet at
GBHS.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
There is ongoing education for staff in the use of personal protective equipment (PPE)
as well as what isolation precautions are needed for a patient with Influenza including a
pandemic. There is ongoing fit testing for staff for N95 masks – done by Occupational
Health Department.
There has been a review of morgue facilities and spaces available in the community
(done by Public Health).
Vaccines will be allocated to the GBHU and distributed to the GBHS based on our
identified numbers of health care workers (provincial plan includes list of priority groups).
Antivirals will be distributed through community pharmacies.
Processes to be implemented:
At Phase 4:
The Incident Management Structure will meet to direct the Directors, Managers and staff
to what is needed to be done for the Pandemic.
Communicate – the GBHS Pandemic Plan with all the stakeholders – i.e. All
Employees, Physicians, Community, EMS, CCAC, etc.
Education of the Pandemic Plan will be done by Infection Prevention and
Control and Occupational Health and Safety for all staff. These departments may be assisted by seconded clinical resources. Physicians, Volunteers, which will include the assessment and triage protocols for influenza-like symptoms, Infection Prevention and Control measures and Occupational Health and Safety measures. This will include the Occupational Health and Safety Committees to ensure that communication will get out to all staff at all sites.
Material Management, Purchasing, Laboratory, Pharmacy, and Food Services
will assess the availability of supplies, equipment and medications needed for the Pandemic response.
The Incident Management Structure will meet to ensure that all plans are in place
and ready to mobilize as needed.
Emergency Information Officer will ensure that communication will be timely,
transparent and accurate to ensure success of our organization's pandemic response as well as dispelling any speculation and incorrect facts that may lead
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
to anxiety and "or operational confusion" – reassuring staff, patients and the public.
Planning Officer – will continue developing their plan based on the current
human resource situation.
Education will continue - to update all employees in new developments, and
decisions that have been made. This will be done by the Public Information
Officer, Infection Prevention and Control, the Nurse Clinicians, Occupational
Health and Safety, and the Directors and Managers.
Consistent information needs to be released so there is no confusion when Phase 6 (Pandemic is upon
us).
Departments i.e. Laboratory, Pharmacy, Diagnostic Imaging, Food Services,
Environmental Services & Dialysis will increase inventory supplies for 4 to 8 week supply over and above what is usually stored.
Material Management will increase inventory supply to 4 to 8 weeks over and
above what is usually stored.
IMS will look at and agree which entrances will be used and which will be closed.
Signage will be ready to be placed strategically to ensure that patients, staff, & visitors know which entrance they need to go to – to be assessed or to be screened prior to entering the buildings.
IMS will decide who will screen patients and visitors coming into GBHS Health
Phase 6 (Pandemic Phase)
The Minister of Health and Long Term Care
will declare a pandemic when it happens.
The Grey Bruce Health Units MOH will notify Health Care Facilities in our area when we
are
locally involved in the pandemic.
The Pandemic plan will be activated to deal with patients, their contacts, employees,
physicians and the community.
The Incident Management Structure will be set up at the call of the Incident Manager or
Administrator on call in the Board Room at the GBHS – Owen Sound site with video
conferencing available for communication with all the sites.
The Incident Management Structure will meet daily or as frequently as necessary to
monitor the hospitals status, supplies, attend teleconferences from Public Health and the
Ministry of Health.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
The GBHS will function normally until the decision is made by the Incident Management
Structure to curtail or cancel services such as: i.e. elective surgeries, ambulatory care
clinics. The decision will be made according to staffing needs and availability of beds.
Day to day hospital operations will continue to provide necessary medical care to those
individuals who present to the emergency department
Key activities will include:
Directors & Department Managers will ensure that the GBHS Pandemic Plan is
available for all staff and is being followed.
Public Information Officer will continue to communicate internally to all
employees and externally to the community by the media.
Infection Prevention and Control will monitor daily Influenza-like illness (ILI)
surveillance reports from nursing units, follow new directives from daily teleconferences and communicate to all staff any new changes that have occurred or are needed for protection.
Occupational Health & Safety will monitor daily staff illness and follow existing
protocols when staff may return to work. They will assist with ongoing employee training, and they will distribute antiviral medication and vaccinations when available to staff and physicians.
At the time of the pandemic, together with the Planning Officer, the Incident
Management will decide if a redeployment centre needs to be activated based on the severity of the situation and the need for redeployment of staff.
Post Peak Period:
At the end of the first wave (Pandemic), it is anticipated there may be recovery
periods to restock and assess situation. The waves may last 4 to 8 weeks and
several waves can be expected.
Need to restock supplies that have been depleted to ensure readiness for the
next wave when it comes
Time for looking at the plan to see if improvements or changes need to be made
– if there were issues that did not work well during the first wave.
Post –Pandemic Period:
The pandemic is over when there have been no new cases presenting.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Need to de-activate the pandemic response activities
Time to evaluate what worked and what did not work to help guide future actions
in identifying "best practices" for future implementation.
Assess the costs associated with the pandemic
Develop a time line for reinstating services that were postponed
Cancel or extend services that were initiated during the pandemic
Evaluate the reporting structure and decision making process that took place
during the pandemic
Demobilize staff and volunteers Formally recognize the efforts of all staff and volunteers
Evaluate immediate & long term emotional needs of staff
Ensure that critical incident and stress management/support is available for staff
Inventory assessment – drugs, assess usage of supplies including patient care
and laboratory supplies, beds, ventilators
Extensively clean and disinfect equipment
Evaluate and summarize the vaccine delivery strategy
Paperwork – staff payroll documentation, activity log records, financial
processing and documentation, seek financial redress,
Communication – the "New Normal", continued promotion of Infection Prevention
and Control and key health messages, the recovery strategy: what to expect, announcements, and notifications of the gradual restoration of services.
Surveillance: estimate burden of disease, revise case definition if necessary,
and evaluate surveillance system and determine ongoing surveillance needs.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
CHAPTER 2: INCIDENT MANAGEMENT SYSTEM
Grey Bruce Health Services recognizes that the success of emergency response
activities is due to an integrated effort by all functional areas of the hospital and its
relationship with external agencies. In order to ensure coordination of GBHS and
community resources allocated to the disaster response effort, GBHS uses the Incident
Management System (IMS) and its principle and establishes an Incident Management
Team, if warranted by the specific situation. As indicated above, the IMS will be
implemented upon notification of WHO phase 4 pandemic if not before.
The Incident Management System (IMS) is an international emergency management
structure that is the recognized North American standard essential for the management
of all emergency incidents. IMS identifies key roles needed to do key functions during a
time of crisis. During a pandemic, the IMS will ensure that resources and skills are
utilized in the most appropriate and efficient manner and ensure that the response is
coordinated and integrated amongst all agencies involved. This framework is position –
driven, not person driven, so that anyone capable can fill the role without having to rely
on specific individuals.
The Incident Management Structure (may be referred to as IMS) This team is made
up of:
The Incident Manager
The Safety Officer
The Executive Officer
The Operations Officer
The Liaison Officer
The Planning Officer
The Emergency Information Officer
The Logistics/Support Officer
The Finance Officer
The Facilities Officer
There are Job Descriptions for each position available which will ensure consistency. These Job Descriptions are found in the Command Center and on the Shared Drive in the IMS folder.

Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
GBHS Staff Roles
During a disaster situation such as a pandemic, all GBHS personnel and designated
medical personnel are considered essential to the operation of the Hospital.
The IMS allows for easy expansion of the basic incident management structure to
include additional personnel assignments designed to accommodate the needs of
specific disaster situations.
All Hospital employees are required to wear their GBHS identification badges at all times
during disaster response activities. Employees who report to the Hospital for disaster
response and are not wearing their Identification will not be granted access to the
hospital.
ID badges may be issued as temporary badges to employees by GBHS Security, once
their identities and role in the response effort has been verified.
Employees who are assigned key roles in the IMS are issued orange position
identification badges designed to clearly identify their role in the response effort. The
person operating in their IMS capacity must wear their IMS identification tag along with
their GBHS tag.
CHAPTER 3: ETHICAL DECISION MAKING
GBHS Pandemic Plan
Ethical Framework.do
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
CHAPTER 4: INFECTION CONTROL
1) Infectivity of the Influenza virus
Influenza is transmitted from person to person when people infected with influenza
cough or sneeze, and droplets of their respiratory secretions are inhaled by the
susceptible host, come into contact with the mucous membranes of the mouth, nose and
possibly eyes of another person. Because the virus in droplets can survive for 24 to 48
hours on hard nonporous surfaces, for 8 to 12 hours on cloth, paper and tissue, and for
5 minutes on hands, people can acquire influenza indirectly by touching contaminated
hands, surfaces and objects. The issue of whether influenza can also be spread by
airborne transmission is controversial. There is no scientific evidence of human-to-
human transmission of influenza by the airborne route. However, available scientific
studies cannot conclusively exclude the theoretical possibility that influenza can become
opportunistically airborne (e.g. during aerosol-generating procedures).
For seasonal influenza, the incubation period for influenza is from 1-3 days. The period
of communicability (duration of viral shedding) continues from 3-5days from clinical
onset in adults and up to 7 days in children. The identification of infected sources may
be difficult as individuals infected with pandemic influenza virus may be able to transmit
influenza up to 24 hours before symptom onset. It should be noted that the actual
virulence, pathogenicity, shedding, incubation period and period of communicability of a
specific pandemic strain of influenza cannot be determined until the pandemic has been
declared and sufficient epidemiologic information has been obtained.
2) Screening and Surveillance
Pre-Pandemic Period:
Currently, GBHS, in keeping with the Ministry of Health and Long-Term Care (MOHLTC)
standards, has an FRI Surveillance Program that consists of two major components:
- Admission screening of inpatients and Emergency patients, and
monitoring of clusters of nosocomial febrile respiratory illness in in-patients and hospital employees.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Febrile Respiratory Illness (FRI) is defined as "all patients who have temperature >38°C AND new or worsening cough or SOB not otherwise explained" The FRI Screening Tool must be completed ASAP on all in-patients, all patients transferred in from other healthcare facilities, and all patents presenting to the Emergency Room. Screening is designed to help health care professionals and organizations identify individuals with a potential FRI who may pose a risk to patients and/or health care providers. Patients presenting with fever and respiratory illness of unknown etiology are immediately asked to:
- Perform hand hygiene - Wear a mask - Wait in a separate area (≥2 meters away from others)
These patients must then be placed on droplet-contact precautions until further information is available. When influenza is suspected or confirmed, the patient must remain on droplet-contact precautions for 5 days after the onset of symptoms, or until symptoms resolve, whichever comes first. Health care providers should consistently use droplet contact precautions when entering the room of patients with symptoms of ILI. The decision to discontinue droplet contact precautions will be determined by the Infection Control practitioner or delegate. Reporting is designed to ensure that information that can be used to identify or follow potential cases of FRI is communicated and shared appropriately, while still safeguarding people's right to confidentiality. The goals are to:
- Maintain a high level of diagnostic suspicion for respiratory viruses and
implement Droplet/Contact precautions immediately
- identify and report all patients who screen positive for FRI - Identify clusters of FRI - Ensure appropriate infection control practices are used for patients who are
admitted to hospital with FRI or who develop FRI while in hospital
- Involve Occupational Health and Safety in a timely manner to insure workers are
- Identify and manage clusters of cases quickly and effectively
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
- Prevent/contain the spread of FRI within the acute care hospital setting - Give public health the information it requires to prevent/contain/manage
community spread
- Internal and external communication is essential to ensure a common
understanding of risks, identify possible clusters or outbreaks in a timely way, and take appropriate action.
The diagnosis of influenza is confirmed by a positive result of a nasopharyngeal aspirate
or swab specimen. In some cases with inpatients, bronchial alveolar lavage specimens
may also be tested for influenza.
Pandemic Period
Influenza during a pandemic is most commonly referred to as Influenza-Like-Illness (ILI).
The actual screening tool that will be used at this time will be determined by the Public
Health Agency of Canada and the Ministry of Health and Long Term Care.
Influenza-Like-Illness: a constellation of symptoms which may be exhibited prior to the
confirmation of influenza. Symptoms include new onset or worsening of existing cough
and/or fever of acute onset >38 C. Other symptoms may include: rhinorrhea, malaise,
rigors or chills, sore throat, headache and myalgia.
Clinical case of influenza: when influenza is circulating in the community, the presence
of fever of acute onset is a good predictor of influenza. The positive predictive value
increases when fever is >38 C and when the onset of illness is acute.
Confirmed case of influenza: those with laboratory confirmation (i.e. virus isolation from
respiratory tract secretions, identification of viral antigens or nucleic acid in the
respiratory tract, or a significant rise in levels of serum antibodies) with symptoms and
an epidemiological link to a confirmed case (Prevention and Control of Influenza during a
Pandemic for All Healthcare Settings, Annex F; May 2011).
Screening will be applied to all individuals wishing to gain access to the hospital
including patients, visitors and staff. Entrances will be limited and secured
It is anticipated that staff will self-screen and only report a new onset of symptoms.
See Chapter 8 – for details regarding staff who screen positive.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Visitor access will be limited as discussed in Chapter 13 Patients entering the hospital for assessment in the Emergency Department or for essential clinical visits will be instructed to:
- Perform hand hygiene - Wear a mask - Wait in a separate area (2 meters away from others) -
These patients must then be placed on Droplet/Contact precautions until further
information is available.
Health care providers must consistently use droplet-contact precautions when entering
the room of patients with symptoms of ILI.
Based on typical influenza epidemiology, Droplet/Contact precautions may be
discontinued 5 days after admission or once ILI symptoms have resolved, whichever
comes first. If there is uncertainty regarding discontinuation of precautions, the Infection
Control Practitioner should be consulted.
Exception: Because of prolonged shedding, immune-compromised oncology patients
should be removed from droplet-contact precautions only in consultation with the
Infection Control Practitioner.
During the pandemic period, surveillance will be conducted in accordance with the
Ontario Health Plan for an Influenza Pandemic (September 2011). The following will be
reported to Public Health: all ER visits for ILI, deaths for which ILI was listed as a
contributing factor on the death certificate, and laboratory-confirmed cases of influenza.
The Ontario Plan recognizes that laboratory capacity for viral testing may be exceeded
in the event of a pandemic and that clinical criteria will likely be the mainstay of
diagnosing influenza. In this event, priority for testing should be given to patients
presenting with atypical symptoms or cases not epidemiologically linked to influenza
In addition to infection control surveillance, Occupational Health & Safety will be required
to report workplace absenteeism rates to Public Health, and the attending physician and
pharmacy will be required to report any adverse events related to antivirals and vaccine
used for pandemic influenza.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Personal Protective Measures
Hand Hygiene:
Hand hygiene is the most effective means of preventing the spread of influenza in both
healthcare and community settings.
1. BEFORE initial patient/patient environment contact
2. BEFORE aseptic procedure
3. AFTER body fluid exposure risk
4. AFTER patient/patient environment contact (Best Practices for Hand Hygiene in All
Health Care Settings, PIDAC 2010).
This can be accomplished through the use of an alcohol-based hand rub or soap and
water if hands are visibly soiled.
Respiratory Etiquette
The following measures to contain respiratory secretions are recommended for all
individuals with signs and symptoms of a respiratory infection:
- Cover the nose and mouth when coughing or sneezing (cough into sleeve); - Use tissues to contain respiratory secretions and dispose of the tissues in the
nearest waste receptacle after use;
- Perform hand hygiene after contact with respiratory secretions or contaminated
objects/materials.
Respiratory Protection
There is no evidence to date to suggest human-to-human transmission of influenza by
the airborne route. Thus, it is recommended that a surgical/procedure mask be used for
respiratory protection for seasonal and pandemic influenza. The decision to wear a mask
(e.g. for droplet protection) or a respirator (e.g. for respiratory protection) when providing
patient care during a pandemic should be based on an assessment of the risk of
exposure to the pandemic influenza viral strain from the patient, the procedure and the
environment as follows:
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
1. Health Care Workers (HCWs) should wear a surgical/procedure mask and face
or eye protection when the HCW will be working within 2 metres of a suspected or confirmed influenza case.
2. HCWs should wear a respirator (N-95) and face or eye protection when the HCW
will be working within 2 metres of the suspected or confirmed influenza patient and the patient is coughing forcefully, the patient is unable or unwilling to comply with respiratory hygiene (e.g., coughing or sneezing into sleeve, using tissue or wearing a mask).A respirator is recommended for all HCWs present in a room when aerosol-generating medical procedures are being performed on a patient with suspected or confirmed influenza (Prevention and Control of Influenza during a Pandemic for All Healthcare Settings, Public Health Agency of Canada; Annex F May 2011). Note: Under most circumstances, the use of N95 respirators is less than ideal because of increased resistance to breathing, dead space and physiologic load, which has been shown to cause hypoxia or headaches after prolonged use. The personal discomfort associated with N95 respirator use frequently results in healthcare workers adjusting the respirator and compromising the face seal to reduce the work of breathing. Studies have clearly shown that N95 respirators worn without maintaining a proper facial seal provide no benefit over surgical masks.
Since there remains a theoretical risk of aerosolization of the influenza virus during certain procedures, an N95 respirator, worn with a proper facial seal, is recommended when performing respiratory procedures that generate droplets/aerosols during an influenza pandemic. These procedures, as defined by the Ontario Provincial Infectious Diseases Advisory Committee (PIDAC), include nebulized therapies, the use of bag-valve mask to ventilate a patient, endotracheal intubation (including during cardio-pulmonary resuscitation), open airway suctioning, tube or needle thoracostomy, bronchoscopy or other upper airway endoscopy, and tracheostomy. Additional guidance on personal protection during procedures that generate droplets/aerosols can be found in (Routine Practices and Additional Precautions in All Healthcare Settings, PIDAC; November 2011). N95 respirators should not be used in community settings, unless respiratory procedures that generate droplets/aerosols are performed (e.g. intubation in an ambulance). Patients with active pulmonary tuberculosis may present with influenza-like symptoms during a pandemic. Patients with suspected pulmonary tuberculosis must be cared for
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
under airborne precautions in a negative pressure room, with use of an N95 respirator
by all personnel in the room.
In designated influenza patient care areas, HCWs may wear the same mask or
respirator between patients if the mask is not compromised in any way (i.e. wet, soiled or
if breathing becomes difficult).Hand hygiene must always be performed immediately
before and after removing a mask or respirator.
Eye Protection
Eye protection should be worn when ever a mask or respirator is worn when providing
care within 2 meters of the patient. This can consist of a mask with attached visor, a
mask plus goggles, or a mask plus a face shield. Eye protection or face shields should
be removed immediately after use and discarded or if eye protection is reusable, place in
appropriate area for cleaning and disinfecting. HCWs should avoid touching their faces
with their hands to prevent self-contamination. Hand hygiene must always be performed
after removing eye protection.
In designated influenza patient care areas, eye protection or face shields may be worn
for sequential care of influenza patients.
Gown Use
Gowns are not required for the routine care of patients suspected or confirmed to have
influenza, unless contact with clothing or skin of the patient or contact with the patient's
immediate (i.e. within 2 metres) environment is anticipated". Long sleeved gowns are
recommended if skin or clothing may be contaminated during patient care. Gowns must
be removed immediately after the indication for their use. Hand hygiene must be
performed immediately after gown removal.
Gowns must be changed between ALL patients. When caring for a number of influenza
patients, gowns MUST be changed between patients, including designated influenza
assessment, admission isolation or cohort areas.
Glove Use
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
As recommended by PHAC Prevention and Control of Influenza during a Pandemic for
All Healthcare Settings; Annex F, May 2011, "Gloves must be worn when coming within
2 metres of a patient with symptoms of ILI. Gloves should be removed and discarded
immediately upon leaving the patient's room or bedspace. Hand hygiene must be
performed immediately after gloves are removed.
When caring for a number of influenza patients, gloves MUST be changed between
patients including within designated influenza assessment, admission isolation or cohort
care areas.
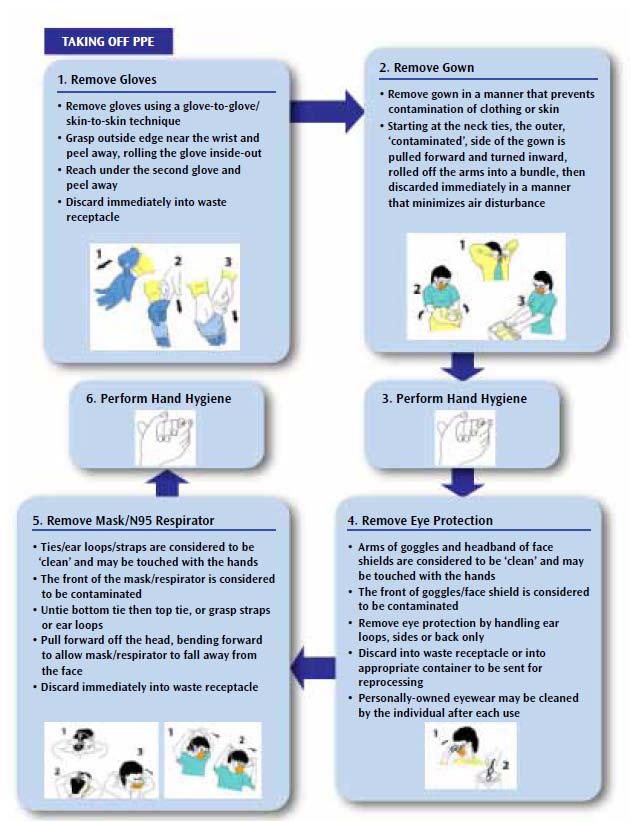
PPE Removal
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
If at any stage of PPE removal staff believe their hands have become contaminated, they should perform hand hygiene before proceeding further
Housekeeping and Disinfection
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
All clutter and entertainment items such as magazines, books, and toys in waiting areas
should be removed to prevent cross contamination and allow for ease of cleaning.
The hospital-approved disinfectant can be used for environmental cleaning as this
product readily inactivates the influenza virus.
Meticulous daily cleaning of all patient care equipment and horizontal surfaces in the
patient's environment is essential.
All contaminated surfaces and equipment should be cleaned following a high risk
procedure. Surfaces and equipment should be disinfected or discarded by staff
performing the high risk procedure before leaving the room and before removing
personal protective equipment. Staff should not re-enter the room until it has been
cleaned.
Non-critical medical devices and medical equipment (i.e. oximeters, IV pumps, armrests,
examining tables, stretchers etc.) should be cleaned and disinfected before use by a
patient and in between patients.
The use of commercial, pre-packaged disinfectant wipes that are easily accessible to all
staff allows efficient cleaning of equipment and surfaces between patients.
Linen, waste, food trays, dishes that are contaminated with secretions from patients with
influenza-like illness symptoms, do not require special handling (Prevention and Control
of Pandemic Influenza in Healthcare Settings, Annex F May 2011).
5) Transport of Patient
The GBHS Infection Prevention and Control policies provide the following
recommendations with regards to a patient being transported who is on Droplet-Contact
Precautions:
- Limit transport of the patient from the room to essential purposes only.
- The patient must wear a surgical/procedure mask when outside of room. When
the patient wears a mask, the HCWs do not need to wear mask and eye protection.
- If the patient is unable to wear a mask or is non compliant, all personnel must
maintain Droplet Contact Precautions.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
The transport worker is to:
- identify the stretcher/wheelchair with the precautions sign, - The transport worker is to wear clean gloves during transport and remove them
and sanitize hands immediately on completion of transport.
- The stretcher/wheelchair is cleaned by Environmental services after transport
6) Education
During the inter-pandemic period, Infection Prevention and Control/Nurse clinicians will
provide the education required for prevention and control of pandemic influenza.
Training will include but not limited to:
Education and skills related to seasonal influenza and pandemic influenza for all
HCWs on all shifts, in all departments.
A review of GBHS pandemic plan, including how it can be accessed
How the organization will communicate their evolving plans during pandemic
An explanation of why and how to perform the daily influenza Self Assessment to
identify ILI symptoms
Infection prevention and control practices to be followed during pandemic,
including appropriate use of PPE
Discussion and explanation of how full application of risk assessment measures,
plus pandemic influenza precautions should minimize or prevent the transmission of all infections, including pandemic influenza
The use of pandemic influenza precautions for all patients with ILI symptoms
Review of strict adherence to hand hygiene
The impact of respiratory hygiene in minimizing influenza transmission
Review known information on current vaccine coverage and antivirals
Education regarding the importance of enhanced (FRI) surveillance in patient
care areas and reporting to infection prevention and control, all new patients exhibiting ILI symptoms
Pandemic influenza education and skills training will be intensified when a
pandemic is imminent.
7) Stockpiling of Supplies
See Chapter 9 – Material Management and Logistical Services for detailed information
regarding the current stockpile of PPE supplies at GBHS.
8) Special Considerations
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
This content of this section was extracted from a document titled "SACC (Scientific
Advisory Committee for Champlain), Response to the Hospitals Working Group Issues
List, March 9, 2007". GBHS supports these recommendations.
Maternal/Newborn Care
The influenza virus may be transmitted to the fetus in utero. However, close contact
between an infected mother and the newborn post-partum will be the more likely route of
transmission.
The virus will most probably be transmitted from the mother to the newborn post-partum
due to close contact, although transmission via breast milk is theoretically possible when
the mother is viremic. This theoretical risk is not a reason to recommend that infected
mothers give up breastfeeding.
Respiratory transmission, not ingestion, is the primary route of transmission.
There are no clinical studies to support the statement that there are harmful effects to
the fetus if the mother is on antivirals because of influenza. Oseltamivir and zanamivir
are considered Category C drugs due to the lack of human safety data in pregnancy.
These medications should be used in pregnancy when the potential benefits outweigh
the potential risk. Zanamivir is considered preferable to oseltamivir for treatment of
pregnant women, unless contraindications to zanamivir exist (e.g. reactive airways
disease), or systemic therapy is required.
All birthing centers should anticipate more preterm labour, but the volume cannot be
accurately quantified. The system's capacity to deal with preterm infants will be limited.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
CHAPTER 5: CAPACITY DETERMINATION, TRIAGE AND BED MANAGEMENT
Triaging- ER patients – Services
Issues Action
-appropriate training for all individuals who
Larger cluster human to human assume it is
will be performing triage
going to progress to pandemic phase and
Communicate with community partners and the
keep talking to staff to allay fears and be
public re: alternate entrance to ED including
location and date this will begin.
No expectation of flu centres in our cities Close relationship required with OH&S to be
aware of the infection rate in our staff
Entering GBHS - Nov2
All patients will be screened using electronic FRI tool increased awareness of ILI and travel history. PPE worn by health care providers.
- Post signs to inform public of alternate entry
Will assume that all patients have been in
contact with ILI
- All patients will be screened using a standard
Insufficient numbers of triage/ED nurses to
screening tool and referred to appropriate level
staff alternate entrance. Consider use of
of care; ED or alternate assessment/treatment
alternate staff to screen i.e. staff from closed
center i.e. ambulatory care department.
programs such as mental health, volunteers.
- PPE worn by health care providers and
screeners. - All patients and visitors will be asked to wear a mask. - all ambulances will arrive through ambulance bay – PPE worn by all staff and patients (as required) all patients screened using FRI tool - Location of triage station will vary depending
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
on location due to physical and flow restrictions:
- OS: tent to enclose front door canopy for
triage before redirecting to ER for other illnesses
- Wiarton: ambulance bay - Meaford: front of ambulatory care - Markdale: registration area tent - Southampton: tent beside the
maintenance building
Lion's Head: Front entrance - Access to the Owen Sound ED bay to be restricted to EMS only. - Limit ED services to patients requiring emergency care i.e. crisis referrals could seen at another location, day surgery visits will not be seen in ED, IV therapies will be treated in the community. - Consider diverting patients to an alternate site if ED becomes overwhelmed. - Redeployment of staff from rural sites will be reviewed by IMS as needed daily to assist with facilitating of services required.
Notes: Consider ER visits to double in Phase 6. This will correspondingly increase our
Med/Surg supplies and drugs (antibiotics for secondary infections)
Critical Care Services
Issues Action
PHASE 4 small cluster human to human
-decide on place to keep the ministry tools and
information on unit for quick reference -Clinical leadership group to discuss provincial plan, affects on GBHS population and Criticall requirements/obligations and SW LHIN One Number Transfer and Repatriation process


Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
flows. -communicate to staff and Patient Movement and Flow Office -review supply, equipment, human resource, capacity plans. This will include critical care and respiratory therapy staff. -communicate this to staff
PHASE 5 larger cluster human to human
contact with tertiary centres to know their
assume it is going to progress to pandemic
status. It is assumed that the MOH will
phase and keep talking to staff to allay fears
utilize critical care bed capacity
requirements as part of the critical care
strategy for the province. This may or may not include access to beds using Criticall and the SW LHIN Patient Access and Flow Transfer and Repatriation process flows.
regular discussions with staff
PHASE 6 Pandemic period
** implement Ontario Health Plan for an Influenza Pandemic July 2007, Chapter 17 Acute care, Critical Care Triage Protocol **
Critical Care Service
Draft Critical Care
Pandemic Triage Proto
Medical Services
Issues Action
- training for non-clinical personnel
(family members, other disciplines, volunteers) - could do personal care, meals, site cleaning, support for health care workers and families so that workers can do their job (i.e. pet or child care),
- Cohort staffing with patients of known
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
- Daily needs and assessment and
- on all admissions with respiratory
symptoms implement Nasal-pharyngeal swabs.
- daily bed rounds needed to be aware of
bed availability and staffing needs (PD, PM, MD, hospitalists, Chief of Service)
- as we are declared to be in Pandemic,
D/C home inpatients with CCAC or when care (self or family) can be safely provided in that environment
- Modification in job duties and schedules
will occur when staff decreases to critical levels
- as demand for inpatient beds increase and
staffing resources shrink:
- adopt clinical care practices to optimize
hospital capacity: provide essential personal care as opposed to full care,
- create "flex beds" from closed beds (i.e.
surgical unit, unused MH capacity
- consider Meaford and Wiarton as
potential expansion sites
- IMS will determine if beds on closed
units can be safely opened and staffed by closing other nursing units or rural sites
- once inpatient capacity is maximized, an
ethical framework will be utilized to ensure fair and equitable allocation of resources with goals to minimize serious illness and deaths.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Women and Child Care Services
Issues Action
PHASE 4 small cluster human to human
decide on place to keep the ministry tools
women who present pregnant and with
and information on unit for quick reference
encourage GP's to utilize "Paediatric
paediatric visits to clinic and ED may
pandemic influenza office assessment form"
display signage from ministry web-site for
children, have paediatric size masks for symptomatic children who cannot be kept 2 metres away from others in waiting areas
PHASE 5 larger cluster human to human
contact with tertiary centres to know their
assume it is going to progress to
pandemic phase and keep talking to staff
regular discussions with staff
to allay fears and be prepared – may see
instruct phone-ins to look at ministry web
increase in visits to ED for children with
site and review "when to seek medical
ED to use ministry tool "influenza
assessment – decision making tool for referral of paediatric patients with influenza-like illness"
PHASE 6 Pandemic period
** see Ontario Health Plan for an Influenza
General information
Pandemic July 2011, Chapter 18, Paediatric
During pandemic, new clinical
Services and Tool (includes Obstetrics) for:
syndromes associated with the infection
may become apparent and a reassessment
Assessment tools
of admission and discharge criteria will
Investigations
It is anticipated that 1/3 of all pregnant
Education and fact sheets
women will experience pandemic
Children will have the highest rates of
attack of influenza and may be the major disseminators of the virus during a
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
pandemic (Local schools may close)
Children aged 6 to 23 months with
certain chronic co-morbid conditions will be at increased risk for complications from influenza.
Early – active in larger centres but not here,
Liaise with area and tertiary hospitals to
we may lose opportunity to transfer Level III
know what is happening in their area and be
mothers and babies and children.
prepared if they become "closed" to
If unable to transfer out we may have
admission for either perinatal or pediatric
higher acuity obstetric cases and babies
and/or children to care for: this will
Birth Prep RN to start preparations for
impact on WCCU nursing, RT,
discontinuing in-house out-patient visits;
physicians, pharmacy, lab, supplies,
include Paediatric clinic secretary in plans
Potential for transfers in from other
hospitals including women, babies and/or children: impact on same group
As it progresses and cases appear locally -
Daily huddles with OB/Paeds and nursing to
Uncomplicated influenza may be similar
establish hotspots and problem solve; to
to the adult disease but there are some
triage admissions (ie OB not admitting,
age related differences in toddlers and
doing electives if nursery is swamped)
Discontinue "Birth Prep" – may continue
Investigations and treatment plans
over phone; discourage outpatient
available from web site – also antiviral
breastfeeding visits and direct to community
medication recommendations for
resources, nurse may do post-discharge
pregnant women with pandemic
influenza – data is limited on safety
Regular contact with PH to stay current
during pregnancy – some women will be
with what is available for new mothers
reluctant to take – risk vs benefit will be
when discharged – this will impact on early
evaluated on individual basis
discharge ability
Paediatric admissions prioritized – some
Relationship impacts: ICU, ED, OR
children will be sent home to be cared for
/PACU, Lab, DI, SPD, housekeeping,
by parents if able/appropriate
pharmacy, IV pumps, supplies, linens,
Keep non-influenza patients separate from
infected patients – isolate all in triage and
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Children admitted to 3-1 or ICU depending
on acuity and in collaboration with ICU, 3-1 staff to support ICU staff as needed/possible
Antepartum women with uncomplicated
influenza – encourage to remain at home and advise re: antiviral medication, hydration, monitoring of temperature, fetal movement counting and when to come to hospital
Intrapartum women to begin or continue
antiviral medication, treat fever, hydrate, use routine practices and precautions, follow usual procedures for intrapartum care
Postpartum women to begin or continue
antiviral medication, treat fever, hydrate, follow standard care for postpartum, continue breastfeeding, isolate if possible, routine practices, discharge early if appropriate
Antepartum with complicated influenza –
hospitalize women who meet the case definition with additional complications. Admissions to ICU in consultation with ICU staff – case by case basis
Intrapartum with complicated influenza –
admission to ICU in consultation with ICU staff – case by case basis.
Postpartum with complicated influenza –
admission to ICU case by case basis and in consultation. Monitor baby continuously. Isolate mother and baby if possible. Discharge when clinically well – may be prior to end of infectious period.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Children with uncomplicated influenza may
be sent home. Resources to support them include education and ministry fact sheets for parents and caregivers to help support them care for sick child at home (available from web-sites)
Early discharge of healthy mother and
Follow-up early discharge by phone,
babies when possible – as early as 6
collaborate with PH – if they stop doing
hours post birth if follow-up available for
home visits, perhaps they will have more
Newborn Screening and Hearing
time for phone visits -
screening otherwise at 24 hours if no PH ability to follow-up at home
Safety to continue breastfeeding
women to be encouraged to continue
unknown until specific pandemic strain
breastfeeding unless strain identified to be
harmful through breastmilk – breastfeeding
women with influenza to be encouraged to take additional precautions such as wearing a surgical mask and practice good hand-washing prior to any contact with the baby
limit family members/visitors to 2
designated people only; limit sibling visits to >10 years of age only and asymptomatic
High rate of admissions possible as both
As nursing and other staff are reduced in
perinatal and paediatric population at risk
numbers, we may require assistance from
– staffing issues on 3-1 – standard
other areas of the hospital. Request from
nurse:patient ratios will be challenged
Human Resources pool.
first and then adequate coverage of the
Triage need for crib and enlist assistance of
unit if high volumes of admissions and
parent with child to use bed with rails up
safely if needed
Challenge if family – pregnant woman
As staffing gets further stretched: look at
with young children – all experiencing
setting up 2 LBR's at postpartum end of hall
pandemic influenza. Most in-patient
so that staff can work more closely and
paediatric have a parent staying with
support each other
them – hopefully families will have a
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
relative/friend who can assist/stay with
Number of cribs available may be
insufficient – we currently have 5
Potential Child-care issues for staff - if
no school and/or if child home sick
Surgical & Ambulatory Care Services
Issues Action
Staffed and Operational
Enhanced - Minor Surge 5%-10%
Surgical services performed at the rural sites will be assessed on a daily basis as per demand.
Augmented – Moderate Surge – 11% - 15%- - Amb Care- continues if possible. If ER at
capacity will close to provide for ER over flow-staff to 4th floor - PSS- continue to see DS
Criteria for cancelling
- DS- this will be decided by the IMS
surgeries and program
- extra staff deployed to HR pool
- PACU-accommodate OR with reduced
- OR-run 4 rooms, DS and Emergencies
- Inpatient Unit-open additional beds as
- Amb Care-closed- area used for ER overflow
Optimum – Major Surge – 16% - 20%
(5 RNs to 6th floor-4 clerical-as needed-
1orthotech to ER)
- PSS-closed- 2 RNs to 6th floor, 3 clerks-as
needed-1 clerk to OR- all staff to be deployed
- DS-closed-redeploy staff to 6th floor-(10
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
nurses- to 6th floor- 1 clerk -1 or attendant –to
OR- all staff deployed to HR pool
- PACU-closed to accommodate CCU overflow
(7 nurses, 1 clerk – stay in overflow – 1 OR
attendant – stay in overflow-all staff to be
deployed to HR pool.
- OR-all elective surgery cancelled- Life or
- Inpatient Unit- open to full capacity
Over Capacity – Large Scale Emergency
- Amb Care-closed – area used for ER over
flow (staff as above)
- PSS-closed- 2 RNs to 4th floor, 3 clerks-as
needed-1 clerk to OR - DS-closed-redeploy staff to 4th floor-(10 nurses- to 4th floor- 1 clerk -1 or attendant –to OR - PACU-closed to accommodate CCU overflow (7 nurses, 1 clerk – stay in overflow – 1 OR attendant – stay in overflow - OR-all elective surgery cancelled- Life or limb only-1-2 ORs staffed and ready-OR staff to assist with surgeries and recover patients - Inpatient Unit- open to full capacity
Notes: With the OR closing their M/S supply budget could be transferred to M/S or ER.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Mental Health Services
Issues Action
PHASE 4 Small cluster human to human
Identify key primary and community
MH services that must be maintained during a pandemic vs those that can be reduced or curtailed.
Identify services that may be in greater
demand during a pandemic (e.g., counseling and support to address pandemic-related fear, anxiety, refusal to work, non-compliance with public health measures, grief and loss) and how they will be delivered.
Identify Pandemic planning binders and
the location of same.
Educate clients about how to reduce the
risk of acquiring influenza and where to go for care.
Identify the type and quantity of
supplies staff will need and potential suppliers for same.
Educate MH staff to the fact that the
recognized assumption is: there will be an increased pressure to provide as much care as possible for people with severe mental illness, to reduce the need for hospitalization.
Identify which health organizations in
the community MH and Addiction Services needs to partner with to provide service. Ie Public Health, CCAC, Social Services, Police Services etc.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Identify possible scenarios and how they
would be handled by the MH System.(e.g., if the hospital has to discharge psychiatric patients, how will the community based programs provide care? Who will dispense medications and how will clients access their medications or be monitored for side effects?)
PHASE 5 large cluster human to human
Support people with influenza who can
be cared for at home.
Encourage staff and visitors to stay
Provide supply kits to MH Community-
Based staff workers.
Maintain the key primary and
community care services during a pandemic.
Contact the Distress Line, operated out
of Ottawa and provide local number for local residents to call.
Assist clients with flu symptoms
connect with flu centres and get the care they need.
Utilize a screening/surveillance
procedure to assess staff, clients and visitors for flu symptoms and implement appropriate precautions (e.g., asking clients with flu symptoms to sit in a separate waiting area or wear a surgical mask)
Work with our community partners
operating residential programs and services that will need to provide some
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
direct care for residents who develop influenza, not requiring hospitalization.
Expect increased demand on
community-based MH services since many people with MH and Addiction problems do not have a primary care provider, and may turn to community-based MH and addiction agencies for care and advice on influenza.
Provide MH and Addiction workers
with knowledge about infection prevention and control to slow the spread of influenza in their congregate living facilities or office-based programs.
See Ontario Health Plan for an Influenza
Pandemic July 2011, Chapter 16, Community-based Mental Health and Addiction Services for posters, assessment tools, treatments, education and fact sheets etc.
Encourage staff, clients and visitors who
have flu symptoms to utilize appropriate services (e.g., Telehealth, flu centres, public health web-sites)
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
PHASE 6 larger cluster human to human
Regular discussions with staff to gather
*assume that 20 to 25% of the mental
their impressions of increased pressure
health and addictions workforce may be
areas and active problem solving
unavailable due to illness, family
Continuation of points listed in Phase 4
responsibilities or other demands in the
Emphasis on containment—Keep non
health care system.
influenza patients separate from infected
patients—reconfigure units to deal with these two different groupings of patients.
Daily short meetings to determine areas
of greatest need and problem solve delivery of service.
Rehabilitation Services
Issues Action
PHASE 5 larger cluster human to human
Screen referrals from non GBHS hospitals for
Assume outbreak of flu is still outside of
flu status in the referring community/hospital.
Grey Bruce area and there is no significant
Consult with Infectious diseases on any
outbreak among staff
questionable cases.
Consider possibility of moving Rehab to another site/location and supply and support requirements to enable this.
PHASE 6 Pandemic period
Discharge all patients who are able to return
home safely (contingent on CCAC support). Limit new intakes to those with the greatest need. Relocate Rehab to another site/location and remain operations as long as sufficient numbers of staff remain healthy. If this is not an option
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
them close to new admissions and discharge patients as soon as possible. Discontinue all outpatient services (including Diabetes Education, Community Stroke Rehab Team and Stroke Clinic) and redeploy staff.
PHASE 6 Pandemic period
Discharge all patients and close unit. Deploy
staff to HR pool.
Oncology Services
Issues Action
PHASE 4 small cluster human to human
Continue to plan. Discuss plans with Material
Assume all staff healthy and outbreak is
Management, DI, Lab and Pharmacy for future
outside of Grey Bruce area
stages of an outbreak.
PHASE 5 larger cluster human to human
Discontinue where possible all 6 month reviews
Assume all staff healthy and outbreak is
based on no exacerbation of symptoms or
outside of Grey Bruce area
significant changes in conditions.
Communicate with London and Toronto
Consider and plan for relocation of service to
Cancer centres to determine the effects of the another area with separate entrance (i.e. 8 units) flu outbreak on their services. Will need to
Need to consider this in concert with Pharmacy
care for increased numbers of sick people
and its plans for this stage and beyond
unable to be seen or cared for in tertiary
Consider using the doctor's entrance for
PHASE 6 Pandemic period
Cancer Care Ontario Pandemic Planning
Guidelines
Communicate with London and Toronto
Cancer centres to determine the effects of the Priority A – Patients who are deemed critical
flu outbreak on their services. Will need to
and require services/treatment even in the
care for increased numbers of sick people
event of a pandemic because their situation is immediately life threatening. Such patients
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
unable to be seen or cared for in tertiary
may need admission depending upon
resources and the severity of the condition.
The important factor is that a patient has a
The program will cease to function if and
condition that is potentially life-threatening.
when insufficient staff members are available
to ensure that all safety standards can be
Priority B – Patients who require
services/treatment but whose situation is
deemed non-life threatening; in the event of a
pandemic, services/treatment could be discontinued for the period of the pandemic wave (8-12 weeks).
Within Priority B, sub-categories of
patients will emerge – patients would receive services/treatment based on availability of resources and anticipated clinical outcomes (i.e. potential for cure adversely affected by delay in treatment; risk to patient if he or she develops influenza during treatment)
Priority C – Patients whose condition is
deemed as non-life threatening who can be deferred, and those services that can be discontinued during the entire pandemic event
Systemic Therapy
New patients who fall into Priority A should continue to be seen to determine if treatment is urgent/curative. Local disease site teams will determine which patients are deemed curative and/or urgent (CCO Priority Categories 1 and 2). New patients who fall into Priority B can
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
be deferred for several weeks. A
mechanism is required (e.g., by phone) to
ascertain that new problems have not
developed if the decision is not to treat
urgently, and for patients to contact the
treatment centre to be assessed if
problems arise (CCO Priority Category 3).
In situations where there are insufficient
resources to treat all curative and/or
urgent cases, patients with life-threatening
symptoms who have potentially curable
cancers will be given priority.
Systemic therapy patient populations
priorities A, B and C
Priority A (CCO Priority Categories 1 and
2)
Those patients being treated who have
aggressive tumours, e.g., some leukemias, lymphomas, CNS, or transplant nd
Patients with life-threatening situations,
e.g., leukemic leucostasis, or medical emergencies such as febrile neutropenia and hypercalcemia
Some patients already receiving
treatment
In situations where there are no hospital
beds, ambulatory treatment strategies
may be required in situations where
inpatient care is the normal approach.
Priority B (CCO Priority Category 3)
The majority of patients requiring
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
chemotherapy (who are not Priority A or C). Recognizing that there is little to no data supporting long delays, this will be a judgment call for each new patient.
Patients already receiving therapy will
need to be assessed as to whether they require ongoing treatment (Priority A) or can possibly wait weeks before continuing treatment.
Priority C
Patients receiving oral hormone therapy, especially in the adjuvant setting
Well follow-up patients
Patients on IV bisphosphonates if that is the only IV treatment required
Unless there is a life-threatening situation,
patients who exhibit influenza symptoms will
not be treated with chemotherapy.
Palliative Care Program
The primary issue when planning for an influenza pandemic is the issue of human resource management. A screening tool would be required to triage patients by telephone. It would be important to identify which patients need to be seen and which patients could be managed via telephone. The telephone will have to be utilized more in the event of a flu pandemic.
In the event of a flu pandemic resulting in limited resources (e.g., physicians, community nurses, and hospital beds), expanding clinic space may have to be considered. This might help to ensure higher efficiency for staff, while utilizing fewer nurses and physicians. The clinic
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
could be supplied with "holding beds" and nasogastric tubes, etc., for use until the patient is stabilized and sent back home. Patients with PPS>60% could be seen in the expanded clinic for assessment. For patients with PPS<50%, consider using symptom response kits in a somewhat expanded version. These would be equipped with the necessities to manage a pain crisis in the home (e.g., sc meds, nasogastric tube for bowel obstruction, expanded sc meds, etc.). Telephone triage could be used to determine if a home visit is necessary
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Diabetes Education
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
CHAPTER 6: LABORATORY/DIAGNOSTIC IMAGING SERVICES
Diagnostic Imaging Services
Issues Action
Review our wait lists for all modalities with
Assuming no staff ill
Central Schedulers and identify how many weeks out we are booking patients. Continue to monitor patients booking schedules and if needed lengthen the time of non urgent appointments to ensure that all urgent cases are completed in a timely manner. No patients will be cancelled at this time. Identify by modality the PPE & essential supplies required for each department.
Assess the lead time of pandemic risk in our
Assumption is that all staff will still be at
region. Staff will need to be educated on the
plan and policies will need to be reviewed. All
departments will review supplies to ensure that we have all essential supplies to maintain the CT, Radiology and Ultrasound departments for life and/or limb cases. All staff will ensure that PPE are available and being used based on the criteria being communicated to department. Central Schedulers will be alerted to potential future need to cancel appointments.
DI services will be under the guidance of the
Early stages – no reported cases in our
IMS committee. DI administration will
participate in regular meetings of the
Operations Group to determine if and when
modalities will be closed to outpatients. The
Chief Radiologist will be consulted. Central
scheduling will be consulted and the booking
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Pandemic stage – cases reported in our
schedules will be adjusted as required.
region. Assumption is that 35% of our staff
DI services will be available for the following
could be affected due to illness or caring for
departments: Emergency, Inpatients and
Surgery. As these departments adjust their
programs DI will adjust accordingly. (IE: not
outpatients)
Close the following modalities:
Bone
Equipment available in DI to be relocated if
needed:
MRI – Anesthetic cart for GA
Nuclear Medicine – Crash cart
Automatic BP machines – Specials, MRI, EDS
and Ultrasound
ALL equipment leaving DI will be marked to
ensure it returns to departments.
Modalities open for "life and limb" only:
Owen Sound – Limited Outpatient services
Radiology will be the only department staffed
24 hours/7 days per week.
Ultrasound will be open for Emergent cases and
OB only - One unit
CT will be available to support the patients still
being seen in the hospital.
C-arm can be set up in a room to be used on
Isolated patients as required.
Two portables will be available to be used
outside the department for general radiography.
Rural hospitals will be open based on the need
and the availability of staff. To be determined
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
by the manager after consulting with the IMS committee. It will be assumed that all patients are infected and full precautions will be applied to all patients. Rooms will be cleaned as needed and as time permits. Detailed instructions will be followed as they are communicated to department. Manager will develop a new staff schedule based on the modalities open and available staff. DI images can be accessed outside of the Hospital for reporting. Any Staff not needed in DI will be deployed to the Human Resources pool. Daily debriefings will be held and staff will be updated via email.
Electro Diagnostic Services
Issues Action
Current phase – Reviewing information and
developing plans. Start adding to regular meetings to educate staff. Determine which modalities will close. Continue to monitor booking schedules. No patient cancellations at this time. Alert Central Scheduling re future cancellations. Identify pressure points – i.e. pacemaker patients who are generally elderly.
Plan and policies reviewed by all staff.
Assume staff will still be at work
Assess lead-time of pandemic risk in our
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
region. Determine at what point to stop booking outpatients. Determine minimum requirements to maintain necessary service -ECG - 2 -ECHO – 1-for emergent scan i.e. pediatric, maybe only on call -Pacemaker – 1-via phone Review supplies needed, PPE required.
EDS services will be under the guidance of the
Early stages – no reported cases in our
IMS committee. EDS administration will
attend regular meetings of the IMS operations
group to determine if and when modalities will
be closed to outpatients. The Chief Internist will
be consulted. Central scheduling will be
consulted and the booking schedules will be
adjusted as required.
Pandemic stage – cases reported in our
Close the following modalities:
region. Assumption is that 35% of our staff
-EEG, EMG, Stress, Holters, AMBP, Loop
could be affected due to illness or caring for
Recorder, 1 ECHO room, Routine Pacemaker
check-ups.
NO OP services except those required for
life/limb, i.e. pediatric ECHO, pre-op ECG,
pacemaker via phone
Equipment available to be relocated if needed:
-ECG machines – 4
-Automatic BP – 1
-Crash cart – 1
ALL equipment leaving EDS will be marked to
ensure it returns to departments
Manager will develop a new schedule based on
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
modalities open and available staff. Any staff not needed in EDS will be deployed to the Human Resources pool
Laboratory
Overview of Pandemic Responsibilities for Laboratory by Phase
WHO Pandemic Lab Responsibility
Phase
Phase 1
Review laboratory preparedness plan, which addresses
laboratory services, operational requirements and human health resources.
Educate and train personnel for pandemic influenza response;
including bio-safety guideline and management of respiratory specimens during an influenza pandemic
Review suspended testing guidelines and testing algorithms.
Maintain essential routine laboratory diagnostic services
Initiate training and cross-training of laboratory personnel in
order to ensure rapid, expert laboratory response, even in the face of decreased number of personnel.
Develop and practice emergency response protocols
Survey all laboratory employees for annual influenza vaccine
uptake and encourage vaccination of all personnel.
Review operational and other plans to manage increased
numbers of requests for influenza testing.
Ensure clearly labeled specimens from patients with
suspected novel influenza are sent to National Microbiology laboratory or Public Health laboratories.
Survey all laboratory personnel for annual vaccine uptake.
Ensure guidelines for specimen type, collection,
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
transportation and testing, as provided by the National and Provincial Pandemic guidelines are implemented.
Review priorities for testing and initiate plan to suspend
testing for non-essential laboratory services.
Enact pandemic plans as needed.
Evaluate pandemic response.
Period: Return to
Revise pandemic response and protocols, as appropriate.
Conduct special post pandemic viral studies, as
Grey Bruce Health Services Laboratory Pandemic Flu Plan
During a Pandemic Influenza Grey Bruce Health Services primary responsibilities are to
maintain laboratory testing services, blood and blood products at appropriate levels. In
order to achieve this we must prioritize and manage the activity of the laboratory staff.
The following are identified risks related to laboratory services during a pandemic:
1. Inadequate laboratory staff to maintain full spectrum of services 2. Inadequate blood product supply from Canadian Blood Services 3. Increased demand on laboratory services 4. Interruption of inventory supplies and equipment support services
Business Continuity
Maintenance of Daily testing:
Decisions regarding laboratory operations will be determined based on Public Health
directives, clinical demands and staffing availability. The laboratory will maintain all
laboratory testing services as long as possible.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
As staffing levels fall, laboratory services will be reduced as listed below:
1. Close all Out Patient Specimen Collection Centers. 2. Reduce Anatomical Pathology services as Operating Rooms close. 3. At a 25% staffing reduction move to Priority 2 = Core services test menu (Appendix A: Test Menu Prioritization by discipline) 4. At a 35% staff reduction move to Priority 1 = Essential services test menu.
Essential service testing will be preserved throughout a pandemic (Appendix A: Test Menu Prioritization by discipline)
5. Contact other laboratory service providers in the region to discuss possible back
up testing services.
6. Plan for offering weekend services 7 days a week in worst case scenario. 7. Inform users or available testing services 8. In partnership with the IMS Operations committee, consider closing one
laboratory (at approximately 20% sick time) then a second laboratory (at approximately 35% sick time).
Human resources:
As staffing levels fall, in an attempt to maintain full spectrum of services and the
increased demand on the laboratory;
Perform an inventory of staffing resources and re-deploy staff as required:
o Re-deploy MLAs as outpatient work is cancelled.
o Deploy staff to alternate sites where feasible.
o Deploy staff across laboratory disciplines where possible.
o If necessary a re-route of specimens or re-route staff can be done.
o Re-deploy clerical staff .
Change length of shifts if necessary to provide suitable coverage. Staff requirements will be assessed on every shift and reduced depending on
Weekend staffing would be in effect during a pandemic event. Redistribute workload across shifts to allow better utilization of off shifts.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Increase all non-full time staff hours.
Equipment and Supplies:
When a Pandemic Alert is identified the Charge technologist or designate must
initiate planning discussions with suppliers to determine if reagents can be sequestered or allocated.
Obtain assurance from suppliers to deliver scheduled and increases in supplies as
Contact courier service to confirm service capacity. Consider collaboration with nearby hospitals in the region in terms of limited
Plan for 1-3 months surplus inventory of selected laboratory supplies
impact on budget Lack of storage Shelf life of supplies
Plan for expanded storage capacity
Infection Control Practices in the Laboratory
To minimize contact, droplet and air-borne or aerosol transmission of influenza
virus when handling specimens, lab staff should adhere to routine practices and additional precautions when appropriate.
o Standard Precautions
Hand hygiene PPE when handling blood, body substances, excretions or
Avoid use of sharps Environmental cleaning Waste management
o Personal Protective Equipment
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Mask Disposable gloves Protective eyewear Long sleeved, cuffed gown
PPE should be worn by all laboratory workers handling specimens from a patient
being investigated for pandemic influenza; and it should be removed prior to leaving the designated laboratory area.
Droplet-contact and air-borne precautions should be employed for procedures
such as manipulating cultures or patient specimens which may result in the generation of aerosols containing virus.
Depending on the available engineering controls, precautions may include the use
of N95 respirators and negative pressure rooms if available.
Biocontainment and Biosafety Guidelines for Laboratories Processing Pandemic
Influenza
Risk assessment governs the level of biosafety and containment required when
handling an infectious organism. The level of biosafety required for the handling and processing of specimens will be assessed and updated as required and guidance provided to laboratories by the province.
Factors which need to be considered included:
o Pathogenicity of the agent
o Consideration of the outcome of exposure
o Natural route of infection
o Other routes of exposure possible resulting from laboratory manipulation
o Stability of the agent in the environment
o Concentration of the agent
o The presence of a suitable host
o Laboratory activity planned (PCR, direct testing)
o Availability of effective prophylaxis or therapeutic intervention
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Containment Levels
For the receipt and processing of human clinical specimens and tissue from
suspicious human novel or pandemic influenza cases Containment Level 2 (CL-2) is required to safely:
o Perform routine diagnostic testing of serum or blood samples
o Perform rapid antigen testing
o Carry out RT-PCR
The primary exposure hazards associated with organisms requiring CL-2 are
through ingestion, inoculation and mucous membrane route. Agents requiring CL-2 facilities are not generally transmitted by the airborne route but care must be taken to avoid the generation of aerosols.
Primary containment devices such as biological safety cabinets and centrifuges
with sealed rotors or safety cups are to be used for CL-2, as well as PPE (gloves, lab coats, protective eyewear).
Transportation:
Packaging, shipping and transport of specimens must comply with the
requirements of the Transportation of Dangerous Good Regulations.
There are daily routine deliveries between facilities with our hospital courier
system, samples and supplies can be transported utilizing the courier.
Stat samples are sent by taxi.
References:
Ontario Health Plan for Influenza Pandemic August 2008
Clinical Health Service Pandemic Influenza Plan, St. Joseph's Healthcare, Hamilton;
April 2008
Pandemic Influenza Plan- The Ottawa Hospital Draft 2; June 29, 2007
Toronto Teaching Hospitals Release Pandemic Influenza Planning Guidelines; May 2006
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Appendix A: TEST MENU PRIORITIZATION BY DISCIPLINE
Priority 1 = Essential services; services to be preserved throughout pandemic (35%
Attack Rates)
Priority 2 = Core services; partially compromised staffing (25% Attack Rates)
Priority 3 = Continue most testing; suspend or reduce routine screening tests to free up
laboratory capacity or address resource shortages (15% Attack Rates)
Essential service - Core Services -
Other Services -
Stat specimens
All bacterial culture
All referred out
Blood cultures
Sterile body fluids
surveillance cultures
serology testing
susceptibilities and
for MRSA and VRE
C. difficile toxin Respiratory screening
for influenza and RSV
Send out respiratory
Morgue/autopsy
Frozen section services
Diagnostic biopsies for
Stat testing
Maintain all testing:
Cold agglutinin
Group and screen
Antibody investigation
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
based on clinical need
Blood and blood product
Priority testing based on:
Urgency (trauma,
bleeding patient)
Non-elective surgery
Oncology as an adjunct
Perinatal needs Pediatric needs
Acetaminophen
Priority 1 Tests plus
Bilirubin, total
Carbamazepine
Ionized calcium
screening tests could
CSF glucose & protein,
Ionized Calcium
HDL cholesterol
Cholesterol Total
Triglycerides
Theophylline
Target Drugs of
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Drugs of Abuse
Glycosylated
ER Drug Screen
Simpli Red D
Urgent peripheral
Urgent bone marrow
Sickle cell screen
Fluids (except for joint) Malaria
CHAPTER 7: PHARMACY
Pharmacy Services
Issues Action
PHASE 5 – Occurring
Keep informed about influenza
Encourage staff to wash hands
Encourage unvaccinated staff to get flu shots
Review Pharmacy Plan regularly
Educate staff on signs and symptoms of influenza Ensure all staff have been fitted for N95
Ensure Pharmacy disaster plan is up-to-date
Ensure multiple pharmacists can sign electronically for
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Develop Pharmacy Critical Drug List
Develop Pharmacy Critical Services list by volumes of staff
required to keep active
Staff to consider limiting travel to effected areas
Review Antiviral stock levels and consider increasing Develop Pharmacy Skeleton staff plans
Ensure security of Antiviral drug stock
Develop plans for antiviral drug distribution link with
Increase critical drug stock on hand from 1 week supply to 1
Phase 5 occurring closer
Establish daily communication plan to keep pharmacy staff informed Staff to implement process changes as required (screening, gowning for deliveries) Order any extra Antiviral stock as required Increase critical drug stock on hand from 1 month supply to 2 month supply Plan for staff and supply shortages Limit vacation time
PHASE 6 – Early
Establish daily communication plan to keep pharmacy staff
informed – Pharmacy leadership
Determine process for determining Pharmacy leadership in
absence of Management staff
Enforce hand washing when entering and leaving the
department Prioritize drug distribution services to critical areas –
Pharmacy leadership. Establish mechanisms for monitoring
volumes of antivirals administered to patients and staff and
create reports to be provided to the MOHLTC.
Reassign unvaccinated staff to duties where they are not
exposed to flu unit – Pharmacy leadership
Review services to determine what are critical services –
Pharmacy leadership
Review hours of operation and determine if remaining staff
can cover – Pharmacy leadership
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Revise shift lengths to ensure staff remaining have adequate
rest – Pharmacy leadership
Consider organizing pharmacy staff into platoons to prevent
crossover infection – Pharmacy leadership Pool pharmacy staffing resources based on site and unit
closures – Pharmacy leadership
Increase ER stock or replace daily to meet needs of
increased ER visits
Implement further security measures for Antiviral stock –
Pharmacy Leadership
Offer surplus pharmacy staff to hospital staff pool –
Pharmacy leadership
Plan for pharmacy drop off zones for medication delivery to
flu units to prevent transmission
Change wardstock system to requisition by nursing
Staff to adapt to working all shift wearing masks
Phase 6 - later
Rural Site techs take on ordering if inventory Tech unavailable Blackberry access to Pharmacy manager if unavailable Transfer drug stock from any closed site to sites remaining in need of supply Pharmacists assist where ever they can – drug distribution, direct Rationing of drug stock where demand outstrips supply – P&T Substitution of one product for another if key drug products unavailable – P&T Support to staff grieving if deaths occur
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
CHAPTER 8: HUMAN RESOURCES
Human Resources:
Phase 1-3
Maintain accurate employee records, producing and auditing reports are necessary
Review HR Section of Pandemic Plan and update as required Cross train HR team on critical HR competencies to ensure appropriate coverage within HR team
Review skills inventory information and decide if it should be updated, if yes, issue skills assessment questionnaire to designated areas Update MediHR with all new skills information
Phase 6 – Implementation
Issues
Action Plan
HR Command Centre
Location: Current HR Offices
The HR Command Centre will be
Services: Redeployment
implemented when the
Resources / Staffing
absenteeism rates reach the point Employee Assistance where managers can no longer
Management Support
staff their unit/area without
external support.
The HR Command Centre will
Command Centre Leader:
report to and work closely with
Chief Human Resources Officer (Designate –
IMS to obtain the following
Manager Human Resources)
information, which is required to
Clinical Leader:
implement redeployment;
Chief Nursing Officer (or Designate)
Support Leader:
- IMS direction on what the
Manager Allied Services & Food Services
essential services will be
Set Up: In existing HR offices and will consist of
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
provided during the
a main reception; central redeployment
meeting area; clinical redeployment
- IMS to define the levels of
office; support redeployment office;
acceptable surge capacity
employee and management support
offices; process control office and a
communication office. Appropriate
clinical and support expertise will be
assigned to the Centre to assist in the
assessment and redeployment of staff
to ensure appropriate skill and ability
match the request for additional staffing
and/or reassignment of staff.
Systems: Current phone lines, computers, fax,
Photocopiers, etc. will be used to
support the team
Communication:
An announcement will be distributed
when the HR Command Centre is
opened advising the location, etc.
Redeployment
Prior to contacting the Command
Redeployment Requests:
Centre for redeployment
assistance, managers are to;
- All redeployment requests are to come into
the HR Command Centre and will be
(1) Continue with their normal
overseen by the HR Command Centre
process for managing
absenteeism; if unsuccessful;
- Managers will be requested to forward their
(2) Send out network messages
schedules via fax or email daily to the HR
requesting staffing support; if
Command Centre showing which staff are
working and which staff are available
(3) Contact the HR Command
- Utilizing the MediHR system which will
Centre Team Leader and
contain the skills and experience inventory
request redeployment
information, reports will be generated as
required for redeployment purposes
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
(4) For internal redeployment,
- Staff will be redeployed as matches are
establish which services will
made to skill, experience and availability
be suspended and in what
- If required, other resource lists will be
utilized to retain additional support, ie.
retirees, students, volunteers, etc.
Redeployment Principles:
The HR Command Centre will
notify IMS when unable to provide During the pandemic staff will be treated as much the resources required and await
as possible in a manner consistent with established
additional direction on essential
Human Resources principles, which respect the
services, base staffing, etc.
core values of GBHS.
The redeployment centre will endeavor to place staff equitably such that workload is shared to the extent it is possible. As much as possible, unionized staff will be redeployed within the context and parameters of the appropriate collective agreement, although this may not always be possible.
Resources / Staffing
- Casual and part-time staff will be contacted
Utilizing all resources and skills
to assess their level of commitment to full
available will be critical to GBHS's
ability to successfully manage the
- Recent retirees contacted to determine their
interest in returning to work during
- Utilize existing students from all clinical and
health care related programs
- Work with Volunteer Services on availability
of GBHS volunteers to determine where their skills could be best utilized
- All new hires during the pandemic event will
be temporary or contract
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
- Nurse educators available for point of care
- NP may be redeployed to support patient
care if MD volumes are reduced
- Department specific critical information
summaries available for redeployed workers
Employee Assistance
Team Leader: Corporate Manager, Organizational
The HR Command Centre will act
Development and Learning
as a central area that all staff can
come to ask questions and
- HR will work with EAP provider to ensure
discuss concerns
additional support is available to staff as required
- A Resiliency Team will be established and
will consist of representatives from HR, OD, professional and clinical practice. This team will address the needs of staff as they may arise from the pandemic (ie. coping mechanisms, stress, etc.)
- Provide information on community
resources that could assist staff during pandemic, (ie. day care, elder care, home pandemic plan, etc.)
Management Assistance and
- HR will provide timely information regarding
all HR, labour relations and safety issues to
During the pandemic managers
management during the pandemic
will require additional support to
- Provide additional support to managers to
deal with not only the staff
ensure they have the tools and information
shortages, increased patient
necessary to deal with staff issues such as,
volumes, but also the impact the
long hours, increased workloads, new work
pandemic will have on their teams. assignments, etc.
Process
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
The HR Command Centre will
- Payroll codes will be established to track
capture, monitor and track all
staff movement as related to the Pandemic
centre activities
(i.e. overtime; reassignment to a department
other than home department, etc.)
- To the extent possible existing policies,
procedures and collective agreements will be followed. Issues that are outside the existing documentation will be reviewed and addresses as they arise.
Communication
Once the HR Command Centre
- During the pandemic HR will work closely
becomes operational a
with the unions to obtain their involvement
communication will be distributed
and input on various issues, in order to
to all staff outlining the location,
where possible, manage the number of
hours, and services provided by
grievances filed
- Communication with managers on the
importance of trying to honour collective agreements, service/seniority and shifts during the pandemic
- Procedures and process communicated on
tracking and paying redeployed workers
Volunteer Services
Issue
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
with severe staff
Occupational Health & Safety - Health Care Workers & Patient Safety and
Support
Staff Surveillance & Screening
Assumptions
Action Plan
Concerns
OH&S committees
responsibilities to
at each site will
from Infection employers to
continue to be
representatives (
protect employees
advisory groups,
from each site or
against health &
during Phase 3, 4, 5
Corporate)on the
responsibilities to all
OH&S committees
to ensure that
employees are
trained &
about the principles
& procedures of
infection control
OH&S committees
review present
policies for
Respiratory
Surveillance &
screening tools,
review Respiratory
Protection program
policy and program
& fit-testing
program ( already
in place)
OH&S committees
Availability
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
involved in plans
for cohorting
patients and
employees
Employees
requiring
restrictions during
a pandemic will
provide OH&S dept
with documentation
to support their
requirement for
eady in place)
When OH&S is
made aware of an
occupational
illness, a WSIB
claim will be filed
During Pandemic:
-OH&S will track HCWs who
report influenza like
report symptoms of acute
Compliance
symptoms(ILI) to
respiratory tract infections
Employee Illness
issues with
-managers will advise OH&S
Reporting forms &
departments
if clusters are observed in
not using the
sore throat, runny
Surveillance form
employee
reporting forms
During Phase 6, 2 types of
-possibly use HRIS
active surveillance will be
system for the data
initiated:
Symptom & Illness tracking,
including RTW info (dept, job
develop data base for
this purpose
-Vaccine & prophylaxis
tracking (dept, job
classification)
Employees who experience
OH&S/ ER at sites
- availability of OH&S
ILI while at work should be
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
assessed by OH&S prior to going home. Assessment to include: - need for lab testing for influenza, -treatment with tamiflu -go to physician -determine whether employee should be sent home
Tracking will be
Screening requirements will
OH&S & Infection
Different surveillance
Screening is
done to identify
Prevention & Control
form than presently
Will continue to track
influenza illness &
employee illnesses.
to determine fitness
to work in different
Screening requirements may
be increased during pandemic
according to MOHLTC
reduce the
risk or
perceived
risk of
spreading
infection to
others in the
hospital
setting
Active
Screening may be
? electronic bar coding of
OH&S & Infection
-need employees to do
Screening
done at the door
HCWs (ie ID badges) for
Prevention & Control
surveillance at entrance,
ideally with linkage to a
shared data base for HR and
Health Records internally, & with potential for inter facility sharing, as required during pandemic
Confidentiality concerns must
be addressed in advance re:
HCW consent to share date
Consent to share info
related to prophylaxis with
related to antivirals
other health care institutions- might be obtained with consent to treatment for
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
antiviral and/or vaccine (already in place)
Management/Decision Support tool to link ICP/HR/OH&S and department within & beyond each facility as may be required
Antivirals &
Vaccine will not be
GBHS will decide who will get Will be dispensed by
available for the first the medication.
need secure
wave of pandemic.
location for
Antivirals will be in
short supply-tamiflu
& zanzmivir (allergy
distribute to
selected staff at
each site.
available. GBHS will OH&S staff will have to be
have to vaccinate
available to provide
Will be done by OH&S
need secure
location for
giving vaccine
to employees at
central location.
i.e. WMP
Staffing clinics
will be a
concern- may
need to recruit
other nurses i.e.
diabetes
educators
Develop a committee with key Use the Quality
Distress
misinformation will
people such as psychiatry,
Worklife Committee,
Management cause anxiety in the
social work, chaplaincy, HR,
supported with the
bioethics, OH&S, EAP
other professions to
provider, frontline staff, senior work on this issue
administration &
attitudinal issues
Need effective communication
& interactive sessions for
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
prevention ie. Vaccination may be avoided due to an unrealistic minimization of infectious threat or by distrust of authorities encouraging vaccination. Need to develop effective & responsive modes of communication within the hospitals & build trust prior to the pandemic's arrival Psychological support in the pandemic phase will be more effective if it is provided through trusted relationships that pre-exist pandemic.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
CHAPTER 9: MATERIAL MANAGEMENT & LOGISTICS
Food Services
Issues Action
PHASES 1,2,3 &4
-Keep informed about influenza
-Encourage staff to wash hands and get flu shots
Communication and Information
-Designate how communication will be done and by
Dissemination to all staff at each hospital site.
whom at each hospital and food service department
- See action plan
-Review pandemic plan with all staff
-Ensure all staff have been fitted for N95
Supplies –
- may be changes in suppliers ordering or
-communicate with suppliers to see if still ordering
delivery systems (may not have online ordering)
on line, delivery dates are still the same
– anticipate less deliveries over time
– write procedure of new ordering system and
- may need to communicate new procedure for
post/communicate to all charge people
-place orders for non-perishables, chemicals and
-will need to increase all non perishables, enteral
disposables to ensure 4 week inventory in stores at
feeds, disposables and chemicals (increase
sanitizer) – need minimum of 4 weeks inventory
- place order for perishables depending on
as long as possible
refrigeration space/code dates safely allows – can
-Increase perishables – bread, milk, dairy as able
use cold beltline room in Owen Sound
- anticipate that # deliveries may start to decrease
Change in Service - Rethermalize food using
-ensure gowns, masks etc are ordered for food
Burlodge Multigens, then assemble trays and
deliver tray rack to Nursing Station.
- Put all disposables for this system into cold beltline room. Rural Hospitals will remain on plated system with the need to go disposable depending on staffing level.
PHASE 5 –
Manager, Supervisors, Lead Hands meet to review
Staffing – how many staff are available to work? staffing available at each site. Review the plan and
Assume 20-25% less staff available as a
how to expedite it. Redo staffing schedules with the
staff available to work.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
- If Aramark hasn't already cancelled all non-
Need to eliminate all non patient related Retail
patient related catering at Owen Sound then GBHS
Food Services will
If not enough FSW for Patient Services –
- establish if Diet Changes, Admissions, Discharges
decision to reduce/eliminate Retail Services
etc. will be through Cerner or other
except for staff working.
May not have Cerner System to interface with
-Establish role of cafeteria space.
Computrition for diet orders – may not have
staffing to enter diets. Establish Clinical Dietitian availability.
Communication – how will Food Services be
- Manager , Supervisor or Lead Hand will be the
communicated to -external to the department and
"Communication Captain" for the department --
internally between the Food Services
Manager or designate to establish what the routes of
Departments and within each hospital site.
communication will be – email, telephone, intranet
- mechanism for communicating with
Occupational Health/Infection Control and
- Manager or charge person to post the pandemic
employees at home to ensure staff are not
plan for staff to follow
reporting to work sick.
-order further supplies (as space allows) to keep
Supplies – assess if have space/mechanism to
inventory as high as possible until no longer able to
order more supplies – dry stores/freezer and
purchase due to shortages or vendor shutdown.
refrigeration.
PHASE 6
Minimum staffing required in Owen Sound –
Staffing – What is the minimum number of staff
Patient Services & essential staff feeding only
needed to run Patient Food Services and essential Manager -1 feeding of staff in all hospital sites?
Supervisor – 1
-what if minimum number of staffing not
available? Keep on china as long as have staff
FSW- 12 (may change depending if on disposables
available for ware washing. Start disposables if
or not) (7.5 hours)
not enough staffing to include ware washing.
Lead Hand/Charge Person-1
Cook - 1 FSW – 2- 3 (7.5 hour shift)
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
- if still not enough staffing for essential feeding–
Retail Service – assess if still needing to feed
Charge person to contact central operations for
staff in their work areas? Any other changes to
redeployment of staff
- move to Emergency Menu (preset menu by
Change in Service – Implement Emergency
supplier) This may need to be adjusted over time if
Pandemic Menu at all hospital sites.
supplies are depleted and are unable to be
-Diet Technician/Supervisor to adjust menu
keeping to therapeutic diets as able
Supplies – some supplies/inventories may be
depleted at some of the sites over time– is the
-charge person to establish transportation of
van system still operating between sites as non-
non-perishables between sites if necessary
perishable supplies may need to be sent by
the van system to the other sites.
-Charge person to keep central operations up to
date on quantities of food available and forecast # of meals still able to produce. In turn central operations needs to let Food Services know changes of service numbers that food must be produced for.
The Following Assumptions Have Been Used:
Aramark Employees (Contract company responsible for Retail Services) may be
negotiated to assist with patient/essential feeding as available.
Food Services will be responsible for delivering food to patients and staff on the units
where they work – Food Services or non-nursing personnel will deliver to the bedside. Therefore will need the appropriate protective equipment ie: masks, gloves, gowns etc.
The cafeterias in all hospital sites may be utilized for other purposes by the hospital.
Patient/staff may need to be fed on trays that have been assembled in the kitchen from
re-thermalized food from Burlodge Multigen Carts
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Our hospitals are only responsible for feeding our patients, staff (priority) and visitors (as
able) and are not a central feeding area for the town/city.
If a hospital site is closed, the food services staff from that site will be redeployed to
other food service departments within the corporation.
The week supply of bottled water and pandemic supply quotas for pandemic menu are in
Material Management
Issue Action
To maintain a four-week supply
of PPE above what the Health
Care Facility would normally
have.
pandemic scenario
Storage space will be an
issue for the extra supplies
An 6 to 8 week supply of PPE's is
stockpiled above what is already in stock
Ministry is stockpiling a
N95 masks will be used during the
four-week provincial
pandemic to ensure safety of our
stockpile of PPE that our
organization will be able to
To access the Ministry stockpile one will
access when/if our
contact the Ministry Emergency Operations
individual/local stockpiles
To maintain other supplies to
function within the Health Care
Facility for 6 to 8 weeks.
Ministry is not stockpiling
Material Management needs to with
direct patient care supplies
assistance from all nursing units,
for the 6 to 8 weeks of the
Pharmacy, Food Services, D.I ,
first wave of the pandemic
Environmental Services, Laboratory,
Respiratory Services, Engineering
Acute Care Requirements
Services, Laundry, Dialysis, Oncology and
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
SPD determine or identify what supplies
Average LOS: 9.5%
will be required to keep the Health Care
Facility running for 6 to 8 weeks
100% using an acute
care bed for 5 days
15% using and ICU bed
7.5 using ventilator
Need to work with Environmental Services
support for 10 days
and /or various suppliers to develop other
Therapy will include
strategies to store products either in a
Oxygen, IV solutions
central location or at the manufacturer's
and Iv antibiotics
Security will be an issue
when one has stockpiled supplies and PPE necessary for Employee protection and supplies to function during a Pandemic event.
Will there be the availability of
Will contact suppliers to see what their
needed supplies?
capabilities will be.
Staffing impact:
There could be 35% of staff Environmental Services:
off ill or home with family
Based on 60% available staffing model,
members who are ill.
only existing inpatient units can be staffed and serviced in OS.
There will be no ES staff available to
support any other program areas unless sites are closed.
Site coverage will only be to inpatient units
and may not be 7 days a week.
May need staff who are redeployed or able
to be redeployed.
Will there be waste disposal or
Our Waste Management
Volumes will be decreased with closures.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
system will be having the
Not all will need refrigeration.
same staffing issues as the
Provision of roll off containers can be
Regular waste – storage on site in roll-off
CHAPTER 10: INFORMATION MANAGEMENT
1) Brief Summary of Unit/Department and General Overview of Impact of
Pandemic
The purpose of the Information Systems Department is to:
• Develop/implement new computer systems, and to
• Provide support for existing computer systems
Our Services:
• Develop, implement and support Clinical Information Systems – Includes Registration
and Ancillary Systems ( Lab, DI, Pharmacy, Health Records etc.), the electronic health
record (Cerner) and Imaging Systems (PACS).
• Develop, implement and support Financial Systems – Includes Ormed Financial
System, Custom Accounts Receivable, and Decision Support Systems.
• Develop, implement and support Material Management Systems – Includes material
management portion of the Ormed System,
• Develop, implement and support Administrative Systems, Human Resources/Payroll
and several departmental administrative systems.
In the event of a Pandemic Flu outbreak the impact to the Information Systems
Department would be "indirect" as we are a service department to the clinical and
administrative programs and do not provide direct patient care. Our full scope of services
may not be available should a significant number of our staff become ill themselves or
unable to come to work due to family.
Patient needs and prioritization of services All seconded clinical resources will be sent
back to their originating department to be deployed as required Potential for assisting with set up of a centralized ESP office to take calls from employees reschedule staff, maintain
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
central log of who is in the building etc. Set up screening areas.
We assume that most project activities will stop therefore staff working on projects may be redeployed outside the Department if not required to support existing systems • All consultant and student activities will cease; consultants and students will be asked to remain at home to reduce the potential risk of spread with the exception of those required to support existing systems • IS support for mission critical systems will be the priority; support for non-critical systems will be provided as resources permit • Staff that are able to provide support from home may be asked to do so, again to reduce the potential risk of spread • We anticipate requirements for some reporting / system enhancements to capture information related to the pandemic both for internal and external purposes. (e.g. new infection control codes in SMS-ADT system). • Consultants* - require only those consultants who are supporting systems.
Challenges in Meeting above needs
The Information Systems Department challenge is in ensuring adequate support for the existing systems and in particular, for those deemed critical to the organization. Staffs supporting systems are not interchangeable; many have expertise in specific areas. For example, business analysts cannot do the work of programmer analysts, and a programmer analyst that supports the financial systems will not have
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
the skills to support the clinical systems.
Issues for Consideration
Issues for Consideration
a) Prioritization of Services
i) Datacentre Operations
• Critical systems will be indentified as
patient care systems or defined as IMS.
• Support methods (remote or local )have
not been identified for each system
• The datacentre may not be equipped to
operate if a critical support mechanism is
impacted.
• IT support staff and vendors may not have
access to the datacentre if the Hospital is
Restricting access to the facilities.
• There are no guarantees that service
providers will respond to onsite support
(fear or lack of resources).
• There may not be adequate infrastructure
capacity to ensure the increased demand
for critical systems.
• There is currently no determination of
what services are not required to be
supported•
All IT support employees currently don't
have access from home for remote support.
This would ensure enough helpdesk
analysts are available to continue providing
adequate support to GBHS employees.
ii) Wide Area Network and Remote
Access Services
• The current remote access infrastructure
may not be adequate sized to support the
increased number of remote access users.
• There is no formalized policy that states
which employees are allowed to work from
home.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
• There is currently no remote access
strategy to deal with the Pandemic. This
would include:
o Guidelines for how employees can be
quickly setup if required.
o Defined standards for home equipment
and services that are essential in order to
gain access to GBHS from home.
External support may be required from an
external screening (tent) on site.
• There may not be adequate vendor
support contracts in-place to ensure
ongoing support requirements are
maintained during the Pandemic.
iii) Helpdesk Operations
• There may not be adequate support staff
available if there is an increase in call
volumes.
• There is no method to decentralize the
helpdesk to allow helpdesk analysts to
work from home if required.
iv) PC Support Operations
• There is no offsite support model where IT
will support employees at their homes.
• Access to certain Hospital areas may not
be available to IT staff.
• There are no contracts currently in-place
to leverage external service providers if
required.
• Critical PC's have not been identified.
v) Videoconferencing Services
• There may not be adequate facilities to
meet the increased demands for
videoconferencing services.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
vi) Voice Support
• Phone system may become unstable /
unavailable due to the increase #'s of calls
to the Hospital.
• There are no current contracts that ensure
the Hospital receives priority services from
telecom service providers.
vii) Call Centre
• Due to the increased call volumes, the call
centre may not be adequately equipped
both Infrastructural and/or staffed to
support the increase call volumes.
• There is no method to allow call centre
employees to work remotely or from home.
We may need to redeploy essential
equipment phones pagers network
wireless, PCs and printers to other
locations as required.
VideoConferencing (OTN)
Will OTN be able to support our
OTN has a comprehensive Pandemic Plan
Will we have enough trained staff to
There is a scheduler at each site. One
schedule cameras and manage OTN
scheduler can make arrangements for the
entire Corporation. OTN Help Desk can schedule in the absence of a qualified scheduler. Schedulers have remote access from home and can view & book on the OTN calendar remotely. There is a need for the scheduler to receive faxed clinical confirmation.
Will we have enough trained staff to
Camera and peripheral inservices are
support cameras administrative use
currently underway. A heightened focus
and peripherals for patient consults
has been placed on all services/departments/users gaining skills and abilities in daily operation of the camera equipment.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
It is anticipated that Telemedicine
A point person at each facility be available
services will be in high demand for
to assist with equipment operation,
patient, informational and
publicizing events as necessary, relay
administrative reasons.
communication to appropriate Teams and continue to offer the normal operational services that GBHS delivers through OTN on a daily basis.
CHAPTER 11: SECURITY, PARKING & TRANSPORTATION
Security:
Issue
Action Plan
Will we have enough staff to
There will not be enough trained staff to secure all
provide security at all sites?
Will there be enough
Redeployed staff could be used to support
the triage or screening areas.
Redeployed staff could aid in giving direction
to staff, visitors and patients
Redeployed staff could be used to unlock
and lock doors etc.
Restricted entrances and exits
Develop a lockdown procedure
will need to be used during a
Only two entrances should be used – main
Pandemic event.
and emergency with both staffed
Appropriate signage will be at these areas to
direct people where to go.
Parking will be free due to lack of staff to
respond to problems/repairs
Security of supplies etc.
During movement of supplies, drugs etc.
Due to shortage of
security will be in high demand.
supplies, vaccine,
Access will need to be tightly controlled to
antivirals etc. security will
labs, material management and pharmacy.
be in high demand.
Transportation of supplies:
Staff who are redeployed from collapsed
Possible shortage of
departments could assist with driving
drivers due to illness
For security issues may need to assign two
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
staff instead of one.
Police assistance may be
Due to illness in their
Will need to be as self sufficient as possible.
department this may be unreasonable
CHAPTER 12: PLANT OPERATION, MAINTENANCE, BIOMEDICAL ENGINEERING
Engineering Services
Issues Action
PHASES 1,2,3 &4
-Keep informed about influenza
During a pandemic, it is expected that
-Encourage staff to wash hands and get flu
additional pressure will be placed on building shots infrastructure that is designed for current
-Designate how communication will be done
capacities only.
and by whom at each hospital
-Review pandemic plan with all staff
-Ensure all staff are respirator fitted
Communication and Information
Supplies –
- may be changes in suppliers ordering or
-communicate with applicable suppliers to see
delivery systems
if ordering process may be affected
– anticipate delivery disruptions
- may need to communicate new procedure
for supply ordering
PHASE 5 –
Manager, Supervisors, Lead Hands meet to
Staffing – how many staff are available to
review staffing available at each site. Review
work? Assume 20-25% less staff available
the plan and how to expedite it. Redo staffing
schedules with the staff available to work.
It is anticipated that no Engineering Service
Department employee's will be available for
deployment to other departments
There are numerous systems and activities
Staff will be assigned to ensure that the
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
that must be maintained during a pandemic
services below are all maintained in good
and are critical to service delivery.
working order during a pandemic and to
resolve issues as they arise.
Emergency Generators & Distribution- the
generators at each hospital provide electrical
power in case of a failure of the main Hydro
One Distribution system. The equipment
connected to the system is limited to life safety
and include, fire alarm, heating systems,
medical gas alarms, vacuum systems, medical
air systems, isolation room fans, emergency
lights. Some areas are fully
serviced by emergency power, OR's, ICU,
PACU, L&D, Emergency and the data centers.
Diagnostic imaging has some equipment on
emergency power.
• Generator Fuel- minimum capacity is 24
hours of continuous service at full load.
Maximum capacity varies per Hospital. Each
location will assess and respond accordingly to
ensure adequate fuel is on hand.
• Fire Alarm System- system monitors all
areas for fire detection and provides early
warning for staff and Fire Department. This
must remain fully functional, staff and
contractor must continue to perform required
• HVAC- used to provide acceptable indoor
climates, heating /cooling / filtering /
(de)humidifying, outside air. Must be
maintained, some spare parts and filters are
stocked in house.
Isolation Rooms- used to isolate a patient.
Lions Head Site: Portable HEPA filtration
unit in the Laboratory
Owen Sound Site: Triage Room, ICU -
3713, 3715, 4-1- 4117, 4119
Markdale Site: One room in Emerg has a
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
portable HEPA filtration unit
Meaford Site: One room in Emerg has a
portable HEPA filtration unit
Southampton Site: One room in Emerg has
a portable HEPA filtration unit
Wiarton Site: One room in Emerg has a
portable HEPA filtration unit
Procedure V-75 provides detailed instructions
for applicable system.
• Medical Vacuum- multiple compressors
systems provide integral backup protection and
are powered from Emergency power
distribution. Markdale system requires
domestic cooling water as well
• Medical Air- similar to medical vacuum,
Owen Sound - yes
Southampton –compressed gas cylinders only
Markdale - compressed gas cylinders only
Meaford – compressed gas cylinders only
Lions Head - compressed gas cylinders only
• Sewage Systems- passive systems are
designed for normal use per building and
• Lighting- Emergency lighting is in place for
• Snow Removal- Contractors for snow
removal will be contacted, priority will be to
maintain service as normal, any reduction in
capability will be agreed upon per Hospital.
• Elevators- Each Hospital has emergency
powered elevator service.
• Oxygen- Bulk and tank oxygen delivery
systems have a main and a reserve supply
sized for normal
Conditions. Pandemic situation requirements
will be analyzed and pro-active supply
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
requirements initiated.
• Heating Systems- facility specific gas, fuel oil
and propane backup must be maintained as
per normal procedures
Communication – how will Engineering
Services communication be executed?
- Manager , Supervisor or Lead Hand will be
the "Communication Captain" for the
department --Manager or designate to establish
what the routes of communication will be –
email, telephone, intranet etc.
- Manager or charge person to post the
pandemic plan for staff to follow
Supplies – assess if have
space/mechanism/need to order more
-order supplies deemed necessary until no
longer able to purchase due to shortages or vendor shutdown.
Minimum staffing required
Staffing – What is the minimum number of
Owen Sound Manager /Supervisors -1
staff needed to maintain operations
Owen Sound Eng. Services - 3
Southampton Eng. Services - 1
Markdale Eng. Services - 1
Meaford Eng. Services - 1
Wiarton / Lions Head Services - 2
-what if minimum number of staffing not
Develop rotating schedule and / or procure
contractor assistance
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
The Following Assumptions Have Been Used:
If a hospital site is closed, the Engineering Services staff from that site will be
redeployed to other Hospital Sites within the corporation.
External utility services (domestic water supply, natural gas delivery, electricity)
will have sufficient contingency provision in place such that delivery of the respective service is functional.
ENVIRONMENTAL SERVICES (Housekeeping, Patient Transport, Inter-Hospital
Courier)
Issue Action
Storage space will be an
Utilize locked storage rooms in Service
issue for the extra
elevator lobby on floor 6, 7, 8 (OS)
supplies needed.
An 6 to 8 week supply of PPE (Disposable
Our organization will NOT be
gowns, Nitrile gloves) stockpiled above what
able to access provincial
is already in stock
stockpiles in a timely fashion
when/if our individual/ local
stockpiles are depleted.
N95 masks (or those recommended by the
MOHLTC) will be used during the pandemic
To maintain other supplies to
to ensure safety of our employees
function within the Health
Care Facility for 6 to 8 weeks.
At PHASE 2; Increase departmental
inventory levels of Disinfectant, cleaning
cloths, ABHR, hand soap, and consumable items to an 8 week supply.
Ministry is not stockpiling
direct patient care
Environmental Services will coordinate with
supplies for the 6 to 8
Material Management to determine or
weeks of the first wave of
identify what supplies will be required to
the pandemic event.
keep the Health Care Facility running for 6 to
Security will be an issue
when one has stockpiled
Need to work with Materials management
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
supplies and PPE
and /or various suppliers to develop other
necessary for Employee
strategies to store products either in a
protection and supplies to
central location or at the manufacturer's
function during a
Will there be the availability of
Will request Materials Management to
needed supplies?
contact Health-Pro / suppliers to see what
their capabilities will be.
Staffing impact:
In the event of Pandemic Influenza, Environmental
Services would need to determine the
There could be 35% of core services that support clinical activity
staff off ill or home with appropriately, and a reduction of non-essential family members who are services would need to occur. This would be ill.
facilitated by an overall reduction/suspension of
Cleaning of rooms and elective surgery, and a decrease/suspension in
equipment from isolated clinic activity. We would anticipate that patients (pandemic) will activity in the Environmental Services department take significantly longer would be reduced time than non isolated patients which will Based on 60% available staffing model, only
negatively affect
existing inpatient units can be staffed and
There will be no ES staff available to support
any other program areas unless Rural Hospital sites are closed.
Site coverage will only be to inpatient units
and may not be 7 days a week.
Will require staff from manpower pool who
have been or are available or able to be redeployed from less critical functions.
Staff from Human Resources pool can be
easily orientated to Routine practices & Infection control concepts using ES tool kit provided by the RICN / Public Health Ontario (approx. 15 hrs required)
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Upon completion of training Redeployed staff
would be buddied with an experienced Environmental Services worker to complete duties as a team
The use of commercial, pre-packaged disinfectant wipes that allows efficient cleaning of equipment and surfaces between patients is to be promoted. PIDAC / Public Health Ontario recommended Best Practices as laid out in the "Best Practices for Environmental Cleaning for Prevention and Control of Infections in All Healthcare Settings (Dec 2009)or subsequent updates shall be followed. The guidelines include the appropriate cleaning agents to use and contact time required to achieve disinfection. ASSUMPTIONS: •Non-unionized employees would be permitted to perform work of the bargaining unit •Part time and casual employees would work 37.5 hours per week •all Unionized employees would be assigned work other than their usual assignment regardless of Bargaining unit or location.
Will there be waste disposal or
Volumes will be decreased with closures.
Our Waste Management
Not all will need refrigeration.
system will be having the
Provision of roll off containers can be
same staffing issues as
arranged from current vendor.
the hospital will.
Regular waste – storage on site in roll-off
Current Vendors;
Explore rental of vehicles to transport waste
Miller Waste (Waste &
Identify vacant buildings that could be rented
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
utilized for off site storage of Bio Medical &
Hazardous waste items to allow for reduced
Stericycle (Bio-Medical, Bio-
frequency / no pick up & disposal available.
Hazardous waste)
Future Environmental (Hazardous waste) The procurement of parts /
Supply chain difficulties may require scavenging
supplies to complete repairs to
from non critical systems if needed
faulty or broken equipment is of
items or services are unavailable
Patient & Material Transport
The movement of patients within
It would be considered a number one priority to
the Owen Sound Hospital is
organize additional staff for Transporting as soon as
dependent on having enough
it was known that a pandemic was imminent. It is a
available staff to maintain patient
function that can be assigned to other employees
following a brief orientation. However, it is an
The process of admission,
assignment that requires direct patient contact and
outpatient and inpatient
there may be higher absentee rate within this group.
diagnostic testing, and
movement in and out of ED and
We would be dependent on the Human Resources
special units can come to a halt if Pool to provide additional employees to support an adequate number of GSW /
Patient / Material Transport .
Transporters/ ORSA's are not
Staff from Human Resources pool can be orientated
to Routine practices & Infection control concepts using ES tool kit provided by the RICN / Public Health Ontario (approx. 15 hrs required) HOWEVER specialized Transport of Patient Infection Prevention and Control Manual provides the following recommendations with regards to a patient being transported who is on Contact-Droplet Precautions: • Limit transport of the patient from the room to
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
essential purposes only. • The patient must wear a surgical/procedure mask when outside of room. When the patient wears a mask, the GSW's do not need to wear mask and eye protection. • If the patient is unable to wear a mask, all personnel must maintain Droplet-Contact Precautions. • The GSW is to identify the stretcher/wheelchair with the appropriate precautions sign, • The GSW is to wear clean gloves during transport and remove them and sanitize hands immediately with ABHR on completion of transport. • The stretcher/wheelchair is brought to the designated area to be cleaned by Housekeeping after transport LINEN DISTRIBUTION: Patient linen, isolation gowns, and OR scrubs are ordered and replenished daily as per the standing orders and a pre-determined schedule. Requests to supplement linen supplies are directed by the end user to the Linen / Laundry Manager. SOILED PICK-UP: Waste, recycling, Soiled linen, reusable procedure trays, patient hardware and soiled equipment is picked up routinely to be brought to various areas in the Level 1 Service area for re-processing (SPD) Transport to Laundry building (soiled linen) or Disposal (waste & recycling). CONTINGENCY CODE RESPONSE GSW's would continue to respond to contingency codes as specified under the relevant Code MAIL SERVICES The daily pick up and delivery of incoming mail from
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Canada Post or inter office mail at the Owen Sound Hospital will be discontinued. Inter Hospital mail and delivery/pickup from Super mailbox (OS Site) will be maintained. Employees will be encouraged to communicate via electronic means whenever possible.
CHAPTER13: VISITORS
In order to minimize the introduction of potential new sources of infection/diseases into
the hospital, it is anticipated that visiting during Pandemic will be significantly curtailed
during Phase 5 and quite likely not permitted at all in Phase 6. In both phases, all
persons entering the hospital will have to be screened for ILI.
CHAPTER 14: COMMUNICATION, EDUCATION, STAKEHOLDER RELATIONS AND
PUBLIC RELATIONS
Vertical Lines of Communication to Activate the Pandemic Plan:
The World Health Organization (WHO) releases an alert about the escalation in WHO
Phases, which is received by national bodies (i.e. Public Health Agency of Canada (PHAC),
Center for Disease Control (CDC) etc.) and available to the public on the WHO website.
PHAC activates the Canadian Pandemic Influenza Plan and the Communications plan
MOHLTC activates Ontario Health Pandemic Influenza Plan through the Chief Medical Officer
of Health, utilizes IMS for the health response, and advises the health system to activate their
plans. EMO activates PCPIP through the Commissioner, utilizes IMS for the provincial
response, and advises municipalities to activate their plans.
Local Public Health Units activate the coordinating pandemic plan with Municipalities and
communicate to the community stakeholders
Community stakeholders (i.e. hospitals may have already activated the plan upon hearing
that the MOHLTC activated OHPIP through the website or an OHA Bulletin) activate their
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Planning Phase
Issues
Action Plan
Internal communications
Organize MOH to provide video conference
sessions to key stakeholder groups.
GBHS staff need a baseline
Create a section on the Intranet for GBHS
understanding of an influenza
Pandemic Information which will include:
pandemic's characteristics,
MOHLTC Public and HCP fact Sheets
clinical protocols, and the
organization's response to
counter any misconceptions or
MOH Presentation
Links to key pandemic information web
Create email question box
Establish Leadership for
Leader is the Public Information Officer
Pandemic communication/
Relief for the PIO needs to be determined
Education
Form Crisis communication Team
Develop Key audience Grid
Ensure Important Health Notices are readily
available to staff on site and at home
Develop ‘New Information template' and
educate about it's location
Create Communications Log
Get Contact information from PIOs in other
organizations to share plans
Develop a Communication
Centralize relevant information on dedicated intranet
Inventory
reference section for pandemic planning to include:
MOHLTC updates
Service Changes
Daily communications
Presentation for Departmental Education
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Develop GBHS communication's clock
Communicating the
Ensure all target groups are identified
Pandemic Plan – how the
Describe the Pandemic planning Process
plan impacts on staff,
Describe decision making process
patients, the public and
Use of IMS structure
other audiences
Availability of information materials
Assess learning/training needs related to
changes in situational requirements or target group- determine timing of required training
Create a training team of those ho are skilled in
training/education to augment those who are in a forma education role.
Educate target groups regarding changes in
protective practices that may occur as new evidence becomes available.
Provide regular training and or up to date
reference materials covering information related to the pandemic.
Pandemic Response:
During the pandemic period, hospital communicators will play a major role in "activating"
the organization's pandemic plan to communicate services/programs (cancellations or
scale-back) changes and what it will mean to staff how operational decisions will be
made during a pandemic (e.g. through the Command centre, using an ethical
framework).
Issues
Action Plan
Disseminating information –
Disseminate information via technical means (emails,
Internal
telephone, and videoconference) to maximize access and
minimize need for person contact.
Have Materials on Hand
Information pamphlets explaining influenza-like illness,
symptoms, self-care
Screening Signage
Visitation Policy
Media Call Sheets
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Self-care for staff
Ensure Key Topics are
1. Issue a daily staff bulletin to communicate operational
covered in regular staff
decisions, new directives and clinical protocols from the
government 2. Share government updates. 3. Convey personal protective instructions 4. Cross-train staff who may be redeployed 5. Work with Occupational Health and Safety Committee to communicate health and safety precautions 6. Ensure communication goes to internal stakeholders first and then gets communicated externally to the public
Continue Communications
Regular updates with communications leads from public
with community stakeholders
health, municipalities, GBHN
and municipal EOC as
Ensure consistency in messages between key organizations
determined in community
Promote annual immunization program
communications plan
Continue communications
Objectives
with public through media,
Ensure quality of communication itself does not become the
web site, joint briefings with
other agency communicators
Drive the communication process proactively rather than
Maintain tight control on who speaks on behalf of the
Utilize the role of the CEO to the maximum
Stay on message. Rigorously brief key officials prior to any
Demonstrate caring about people. Recognize public anxiety,
don't dismiss it
Actions - Public
1. Update public when services are decreased or suspended
2. Where to go for further information : 24-hour public
information line, website, fact sheets and Telehealth Ontario
3. Communicate how to minimize the spread of infection
4. Share the most recent information from the MOHLTC
Key Messages should express:
1. Expression of empathy with worries/fear
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
100 of 106
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
2. Confirmation of the known facts 3. Description of what is known and not known 4. Steps taken by the hospitals to address unknowns and
impact on services
5. Statement of commitment
Actions - Media
1. Identify local papers and health reporters
2. Dedicate a media line to ensure timely triaging and
resolution to all media calls
3. Develop job aids and/or scripts to assist front line staff in
dealing challenging situations related to pandemic communication
Support front line staff in
Ensure communications staff and other front line staff are
dealing with patient and the
supported in their communication with others (dealing with
difficult people and situations
Information Cycle
Understand the timing of the Ministry of Health's 24 hour
information cycle in order to anticipate new directives and
updates, and anticipate the day's focus of media coverage
Develop GBHS information ‘clock' incorporating the
MOHLTC and OHA information cycles
Ensure target groups have up to date knowledge of plans,
risks and responsibilities related to their prevention from spread of infection.
Ensure Provincial preparedness plan is accessible to staff
Materials and Training for staff
Assessment protocols for influenza-like symptoms:
Infection Prevention and Control measures
Occupational Health and safety measures
Provide training and up to date reference materials covering
information related to the pandemic.
Ensure staff/volunteers maintain current and accurate
knowledge regarding containment strategies.
Ensure staff and volunteers are aware of the importance of
anti viral prophylaxis, immunization, including side effects and benefits.
Cross-train staff who may be redeployed, at least annually or
more frequently if threat of pandemic is imminent
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
101 of 106
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Increase services provided by external EAP provider in
addressing staff/caregiver stress management to maintain resiliency
Inter-pandemic Period
Communication will support staff, patients and the public in revering from the pandemic.
Need to include communication efforts to explain the rationale behind the
organizations/pandemic response (e.g. cancellation of elective surgeries, staff
redeployment, priority groups for anti-virals), recognition of the contributions made by
staff/volunteers/students, and the organization/s resumption of services and programs.
Evaluate the communication strategy-its success and weaknesses, as well as identify
and "lessons learned" to guide communication plans for future emergencies.
CHAPTER 15: POST PANDEMIC PERIOD
The majority of this content has been extracted from the Ottawa Hospital Pandemic
Influenza Plan Draft # 2, June 2007. This will serve as a guideline in addition to post-
pandemic planning that will be done by each department/program. The primary focus of
work during the post-pandemic period is to de-activate the pandemic response activities,
review their impact and examine lessons learned to guide future planning for the
potential second and third waves of the pandemic. The pandemic wave may sweep
across Canada in one to two months affecting multiple locations simultaneously; the
influenza pandemic may occur in two or more waves lasting six to eight weeks in any
locality. Overall, the pandemic may last 12 to 18 months and more than one wave may
occur with a 12 month period (Prevention and Control of Influenza during a Pandemic for
All Healthcare Settings, Public Health Agency of Canada; Annex F May 2011).
The pandemic will have a profound affect on health care workers; therefore this recovery
period is essential to ensure the welfare of staff.
A post-pandemic plan is required to outline how to scale back activities and measures
that were implemented during the emergency. Guidance on activities that should be
maintained and those that can be scaled back during the recovery period will ensure a
consistent response and help to focus limited resources. In addition, those services that
were scaled back will have to be reevaluated and slowly return to their regular service
levels.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
102 of 106
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Restoring Services
Recovery needs to coordinated, comprehensive and have a clear strategy. The recovery
plan should identify resources and define responsibility for the range of specific services
to be provided. The following elements should be addressed as part of a recovery
strategy:
Facility:
Demobilize/re-evaluate security services
Access costs associated with the pandemic
Project when GBHS will be able to resume pre-pandemic services
Review/revise clinical management guidelines Review/revise Infection Prevention and Control Guidelines
Evaluate the reporting structure and decision-making process that took place
during the pandemic (IMS)
Review the response plan and draft a lessons learned report
Update Pandemic Plan based on updated guidelines and lessons learned
Reinstate services that were postponed
Cancel or extend services that were initiated during the pandemic
Determine if patient's services need to be re-evaluated as a result of pandemic Determine if new services are required long term as a result of pandemic
Human Resources:
Demobilization of staff and volunteers
Formally recognize the efforts of all staff and volunteers
Evaluate immediate emotional needs of staff
Evaluate long term emotional needs of staff
Evaluate the use of psychological and social services for staff
Ensure that critical incident and stress management/support is available for staff
Paperwork:
Staff payroll documentation
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
103 of 106
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Activity log records
Financial processing and documentation
Seek financial redress
After-action
Communication:
To acknowledge contributions of all stakeholders in managing the pandemic
To provide information on the re-establishment of services that were temporarily
To make all people aware of uncertainties associated with subsequent waves
To evaluate and update the communications strategy
Inventory Assessment:
Assess usage of supplies including patient care and laboratory supplies and re-
stock adequately
Develop projections for future requirements
Equipment:
Determine if items have been rented, leased, borrowed and need to be returned
Determine if GBHS has loaned out equipment and ask for return
Repair or replace any damaged equipment
Replace lost equipment
Extensively clean and disinfect all equipment
Antivirals:
Evaluate the effectiveness of the antiviral strategy
Summarize adverse events data Perform an inventory assessment
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
104 of 106
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Vaccine:
Evaluate and summarize the vaccine delivery strategy
Summarize adverse event data
Perform inventory assessment
Surveillance:
Estimate and summarize burden of disease
Revise case definitions if necessary (based on recommendations from
Evaluate surveillance system and determine ongoing surveillance needs
GLOSSARY
Glossary
Cohort
Two or more patients exposed to or infected with the same organism who are separated
physically (e.g. in a separate room or to one ward) from other patients who have not
been exposed to or infected with that organism. Designating equipment to be used only
with influenza patients. Bringing services to them (i.e. portable x-ray equipment).
Cohort staffing
The practice of assigning specified personnel to care only for patients known to be
exposed to or infected with the same organism. Such personnel would not participate in
the care of patients who have not been exposed to or infected with that organism.
Cohort recovered staff to care for influenza patients.
Contact transmission
Includes direct contact, indirect contact and droplet transmission as described below:
Direct contact occurs when transfer of microorganism results from direct physical contact
between an infected or colonized individual and a susceptible host.
Indirect contact involves passive transfer of microorganisms to a susceptible host via an
intermediate object such as contaminated hands that are not washed between patients
or contaminated instruments or other inanimate objects in the patient's immediate
environment.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
105 of 106
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Droplet refers to large droplets, greater than or equal to 5 um in diameter, generated
from the respiratory tract of the source patient during coughing or sneezing, or during
procedures such as suctioning or bronchoscopy. These droplets are propelled a short
distance, less than 1 meter, through the air and deposited on the nasal or oral mucosa of
the new host.
Fit for Work
Terminology used in occupational health to communicate a worker's ability to remain
/return to work:
Fit for work, unfit for work, fit with restrictions allows the Occupational Health Nurse to
maintain confidentiality about workers diagnosis, symptoms, immune status, etc.
Fit for Work – fit to work with no restrictions
Unfit for Work- defined as a medically determinable illness that prevents an employee
from performing the regular or modified duties of their occupation.
Fit for work with restrictions – Allows for reassignment of duties or reintegration into
the workplace in a manner that will not pose an infection risk to the HCW or to the
patients and or other individuals in the workplace.
Influenza
Clinical Case Definition of Influenza
When influenza is circulating in the community, the presence of fever and cough
of acute onset are good predictors of influenza. The positive predictive value increases
when fever is higher than 38 degrees Centigrade and when the time of onset of the
clinical illness is acute (less than 48 hours after the prodromes). Other symptoms, such
as sore throat, rhino rhea, malaise, rigors or chills, myalgia and headache, although
unspecific, may also be present.
Confirmed Case of Influenza
Confirmed cases of influenza are cases with laboratory confirmation (i.e. virus isolation
from respiratory tract secretions, identification of viral antigens or nucleic acid in the
respiratory tract, or significant rise in serum antibodies) or clinical cases with an
epidemiological link to a laboratory confirmed case.
Grey Bruce Health Services
Contingency Planning
Category:
Pandemic Influenza Plan
106 of 106
Issued By:
Executive Committee
Date of Issue:
Reference:
Ontario Pandemic Plan 2008
World Health Pandemic Plan
Canadian Pandemic Plan 2011
OHA Pandemic Toolkit for
Small, Rural and Northern
Dec. 2007 Mar. 2008 Sept. 2012
Influenza-like-illness (ILI)
For surveillance purposes, the ILI definition currently used in Canada says:
Acute onset of respiratory illness with fever (>38 degrees C) and cough and with one or
more of the following: sore throat, arthralgia, myalgia or prostration, which could be due
to influenza virus. In Children under 5 gastrointestinal symptoms may also be present.
In patients under 5 or 65 and older, fever may not be prominent. Source: Fluwatch
(national case) definition for the 2006-2007 season.
Infectivity of the influenza Virus
Incubation period: 1-3 days
Period of communicability: Infectious 1 day before onset of symptoms and may be
longer than 7 days after the onset of symptoms. Adults are infectious for 3 to 5 days
after symptoms appear while children are infectious for up to 7 days.
Influenza-like Illness Assessment Tool
Influenza-like illness in the general population is determined by the presence of 1,2 and
3 and any of 4, a-d which could be due to influenza virus:
1. Acute onset of respiratory illness 2. Fever (> 38 C) 3. Cough 4. One or more of the following:
a) Sore throat b) Arthralgia c) Myalgia or prostration d) Diarrhea can be a symptom with children
The elderly may not have a temperature.
Source: https://gbhs.on.ca/photouploads/GBHS%20Pandemic%20Plan.pdf
Inscrita el 11/10/2001 con el número 255 en el Registro de ICC Extranjeras de la CNMV MEDIOLANUM INTERNATIONAL FUNDS LIMITED (Sociedad Gestora) RBC DEXIA INVESTOR SERVICES BANK S.A., DUBLIN BRANCH ESCRITURA DE TRUST MODIFICADA Y REFUNDIDA (un fondo de inversión en régimen fiduciario ("unit trust"). DILLON EUSTACE SOLICITORS
Safe Design of Custom Lithium Batteries By Paul Edwards, Steatite Batteries Introduction: The World's Favourite Battery Chemistry? Lithium battery technology is often preferred for portable equipment intended for use in harsh environments. Lithium batteries also have a wide operating temperature range, particularly at low temperatures, and are known to have high tolerance of pressure, shock and vibration. The batteries are







