Igg4 cholangiopathy â€" current concept, diagnosis, and pathogenesis


Clinical Application of Basic Science
IgG4 cholangiopathy – Current concept, diagnosis, and pathogenesis
Kazuichi Okazaki⇑, Kazushige Uchida, Masanori Koyabu, Hideaki Miyoshi, Tsukasa Ikeura,
The Third Department of Internal Medicine, Division of Gastroenterology and Hepatology, Kansai Medical University, Osaka, Japan
levels of IgG4 , massive infiltration of IgG4-positive plasmacells with storiform fibrosis and/or obliterative phlebitis in the
IgG4 related cholangiopathy, a distinctive type of cholangitis of
bile duct wall and good response to steroids Patients with
unknown origin, is characterized by increased serum levels of
IgG4-cholangiopathy are frequently associated with autoimmune
IgG4, massive infiltration of IgG4-positive plasma cells with
pancreatitis (AIP) , the concept of which was originally pro-
storiform fibrosis and/or obliterative phlebitis in the thickened
posed by Yoshida et al. and Hamano et al. reported increased
bile duct wall, and good response to steroids. Patients with
serum levels of IgG4 in Japanese patients with AIP . Now, it is
IgG4-cholangiopathy are frequently associated with autoimmune
recognized as a biliary manifestation of IgG4-related disease
pancreatitis; IgG4-cholangiopathy is recognized as a biliary man-
(IgG4-RD) . Clinically, it is important to distinguish IgG4-
ifestation of IgG4-related disease. This condition can be diagnosed
cholangiopathy from malignancy such as cholangiocarcinoma,
by a combination of imaging, serology, histopathology, and
pancreas cancer, or a benign counterpart, PSC The organizing
steroid responsiveness; however, cholangiographic features are
committee of the first international symposium on IgG4-RD in
often difficult to differentiate from primary sclerosing cholangitis,
2009 proposed the nomenclature of ‘‘IgG4-related sclerosing
pancreatic cancer, or cholangiocarcinoma. The Japanese clinical
cholangitis'' (IgG4-SC) instead of ‘‘IgG4-associated cholangitis''
diagnostic criteria for IgG4-related sclerosing cholangitis estab-
which was recommended by the European Association for the
lished in 2012 are useful in the diagnosis of IgG4-cholangiopathy.
Study of the Liver (EASL) . Recently, the Japanese clinical
Although the precise pathogenic mechanism remains unclear, the
diagnostic criteria 2012 for IgG4-SC have been proposed,
development of IgG4-cholangiopathy may involve: susceptible
although the pathogenic mechanisms remain unclear . Here,
genetic factors, abnormal innate and acquired immunity,
we introduce the current concept, diagnosis, and recent advances
decreased naïve regulatory T cells, and specific B cell responses.
in the pathogenesis of IgG4-SC.
Further studies on genetic backgrounds, disease specific anti-
gens, and the role of IgG4 are necessary to clarify the pathogenesis.
Ó 2014 Published by Elsevier B.V. on behalf of the European
Current concept and diagnosis of IgG4-SC
Association for the Study of the Liver. Open access under
Classification of sclerosing cholangitis
Sclerosing cholangitis is classified into a primary type of
unknown origin such as PSC or IgG4-SC, and secondary type with
obvious pathogenesis (e.g., common bile duct (CBD) stone, chol-angiocarcinoma, trauma, operation of biliary tract, congenital
IgG4 related cholangiopathy is a distinctive type of cholangitis of
biliary anatomy, corrosive cholangitis, ischemic bile duct steno-
unknown origin, which is characterized by increased serum
sis, AIDS-related cholangitis, or biliary injury of intra-arterialchemotherapy) ().
Keywords: IgG4-related disease; IgG4-cholangiopathy; IgG4-related sclerosingcholangitis; Autoimmune pancreatitis.
Received 31 October 2013; received in revised form 23 March 2014; accepted 7 April
Prevalence of IgG4-SC
2014⇑ Corresponding author. Address: The Third Department of Internal Medicine,Division of Gastroenterology and Hepatology, Kansai Medical University,
The prevalence of IgG4-SC still remains unclear. About 80% of AIP
Shinmachi, Hirakata, Osaka 573-1197, Japan. Tel.: +81 72 804 0101x3223; fax:
patients suffer complications with stenosis of the distal CBD with
+81 72 804 2061.
wall thickness This stricture might be due to both the
E-mail address: (K. Okazaki).
Abbreviations: AIP, autoimmune pancreatitis; ANA, anti-nuclear antibody; CA-II,
thickening of bile duct and the effect of inflammation and/or
carbonic anhydrase-II; CBD, common bile duct; CTLA-4, cytotoxic T lymphocyte
edema of pancreas without CBD wall thickness. Based on these
antigen-4; ERCP, endoscopic retrograde cholangio-pancreatography; FCRL,
propositions, a recent Japanese national study analyzed 197 PSC
and 43 IgG4-SC patients without AIP The male/female ratio
IgG4-SC, IgG4-related sclerosing cholangitis; IL-4, interleukin-4; LF, lactoferrin;
was 106:91 (1.16:1) in PSC and 33:10 (3.3:1) in IgG4-SC and
LPSP, lymphoplasmacytic sclerosing pancreatitis; PSC, primary sclerosingcholangitis.
the mean age [min–max] was 48.1 [4.0–86.3] in PSC and 69.3
Journal of Hepatology 2014 vol. 61 j 690–695

JOURNAL OF HEPATOLOGY
Table 1. Classification of sclerosing cholangitis.
(. Type 1 IgG4-SC shows stenosis only in the distalCBD, which is often observed in pancreas cancer. Type 2 IgG4-
Sclerosing cholangitis of unknown origin
SC, in which stenosis is diffusely distributed throughout the
Primary sclerosing cholangitis (PSC)
intrahepatic/proximal bile ducts, should be differentiated from
IgG4-related sclerosing cholangitis (IgG4-SC)
PSC. Type 3 and type 4 of IgG4-SC show stenosis in the hilar
Secondary sclerosing cholangitis
hepatic bile duct similar to hepatic hilar cholangiocarcinoma.
Biliary lesion in AIDS patients
Circular/symmetric thickening of the bile duct
Circular and symmetric thickening of the bile duct wall, smooth
Postoperative/bile duct injury
outer and inner margin, and homogenous internal echo demon-strated by abdominal ultrasonography (US), abdominal computed
Congenital biliary disorders
tomography (CT), abdominal magnetic resonance imaging (MRI),
Chemical agents/drug-induced cholangitis
endoscopic ultrasonography (EUS), and intraductal ultrasonogra-
Ischemic biliary stenosis
phy (IDUS) are most characteristic images of the bile duct
These characteristic features are recognized not only in thestenotic areas or occasionally in the gallbladder but also in areaswithout stenosis that appear normal in a cholangiogram .
[47.6–87.4] in IgG4-SC . Cholangiographic classification of
Characteristic hematological findings
IgG4-SC () according to the clinical diagnostic criteria ofIgG4-SC in 2012 demonstrated that type IV, in which stric-
More than 80% of the patients with IgG4-SC show elevation of
tures of the bile duct are detected only in the hepatic hilar lesions
serum hepatobiliary enzymes, total bilirubin in cases of
similar to cholangiocarcinoma was the most common in cases of
obstructive jaundice, and serum IgG4 levels (higher than the
IgG4-SC without AIP .
upper limit of normal value (ULN) of 135 mg/dl) However,elevation of serum IgG4 levels is not necessarily specific to
Bile duct images of IgG4-SC
IgG4-SC; it is also observed in atopic dermatitis, pemphigus,asthma, and some malignant cholangio-pancreatic diseases
Cut-off values of serum IgG4 higher than x 2 ULN may
Four types of the characteristic cholangiographic features of
be useful for more precisely differentiating IgG4-SC from PSC or
IgG4-SC have been proposed based on the regions of stricture
Pancreatic cancer
Primary sclerosing cholangitis
Gallbladder cancer
Chronic pancreatitis
IDUS* (bile duct)
EUS (bile duct, pancreas)
EUS-FNA** (pancreas)
Colonoscopy (R/O co-existence of IBD***)
Biopsy (bile duct)
Biopsy (bile duct)
Fig. 1. Classification of cholangiography in IgG4-related sclerosing cholangitis. The characteristic features of IgG4-SC can be classified into 4 types based on the regionsof stricture as revealed by cholangiography and differential diagnosis. Type 1 IgG4-SC shows stenosis only in the lower part of the common bile duct, and it should bedifferentiated from chronic pancreatitis, pancreatic cancer, or cholangiocarcinoma. Type 2 IgG4-SC, in which stenosis is diffusely distributed throughout the intrahepaticand extrahepatic bile ducts, should be differentiated from PSC. Type 2 is further subdivided into 2 types. Type 2a, with narrowing of the intrahepatic bile ducts withprestenotic dilation and Type 2b, with narrowing of the intrahepatic bile ducts without prestenotic dilation and reduced bile duct branches, which is caused by markedlymphocytic and plasmacyte infiltration into the peripheral bile ducts. Type 3 IgG4-SC is characterized by stenosis in both the hilar hepatic lesions and the lower part ofcommon bile duct. Type 4 IgG4-SC shows strictures of the bile duct only in the hilar hepatic lesions. Cholangiographic findings of type 3 and type 4 need to be discriminatedfrom those of cholangiocarcinoma. ⁄IDUS, intraductal ultrasonography; ⁄⁄EUS-FNA, endoscopic ultrasound-guided fine-needle aspiration; ⁄⁄⁄IBD, inflammatory boweldisease. Modified from Hepatobiliary Pancreat Sci. 2012;19:536–542 , Copyright Ó 2013, with permission.
Journal of Hepatology 2014 vol. 61 j 690–695

Clinical Application of Basic Science
Other organ involvements (OOIs)
histocompatibility complex (HLA-DRB1⁄0405-DQB1⁄0401), poly-morphisms of nuclear factor-jB and Fc-receptor-like (FCRL) 3
Most cases of IgG4-SC (80–90%) are associated with AIP. It is
genes expressed on B cells have been reported in the Japanese
particularly difficult to accurately diagnose IgG4-SC without AIP
patients with AIP .
. Occasionally, IgG4-SC is associated with other systemicIgG4-RD such as IgG4-related symmetrical dacryoadenitis/sialad-
enitis and IgG4-related retroperitoneal fibrosis ; these arehelpful in the diagnosis of IgG4-SC. Unlike PSC, inflammatory
Recently, abnormal innate immunity has been demonstrated in
bowel disease (IBD) is rarely observed in patients with IgG4-SC
patients with IgG4-RD. Activation of NOD-2 and TLR ligands on
monocytes or basophils from patients with IgG4-related AIPenhance IgG4 responses via B cell activating factor (BAFF) and
Histopathological findings of bile ducts
IL-13, although specific pathogens still remain unclear Inanimal models, activation of TLR3 (polyinosinic:polycytidylic
In IgG4-SC, massive infiltration of IgG4-positive plasma cells, sto-
acid) or TLR4 (LPS) can induce immune-mediated cholangitis,
riform fibrosis, and/or obliterative phlebitis in the bile duct wall
pancreatitis, and sialadenitis similar to human IgG4-RD
are characteristic and called lymphoplasmacytic sclerosingcholangitis (LPSC) Such fibroinflammatory involvement is
mainly observed in the submucosa of the bile duct wall, whereasthe epithelium of the bile duct is intact Endoscopic transpap-
Role of IgG4 in IgG4-SC
illary bile duct biopsy or cytological examinations are useful for
Although the association of IgE-mediated allergy and IgG4 anti-
differential diagnosis of cholangiocarcinoma, although it is diffi-
bodies is well known, IgG4 characteristics are still poorly under-
cult to take enough biopsy samples for characteristic histopathol-
stood. IgG4 has non-acting characteristics for immune responses,
ogical findings of IgG4-SC . Liver biopsy is sometimes useful in
and is involved in a continuous process referred to as ‘Fab-arm
the diagnosis of IgG4-SC in cases of intrahepatic bile duct
exchange', which is a swapping of a heavy chain and attached
involvement .
light chain (half-molecule) with a heavy-light chain pair fromanother molecule; this usually results in asymmetric antibodies
Effectiveness of steroid therapy
with two different antigen-combining sites While these mod-ified antibodies are hetero-bivalent, they behave as monovalent
In contrast to PSC or cholangiocarcinoma, the most characteristic
antibodies. Another aspect of IgG4 is that it mimics IgG rheuma-
feature of IgG4-SC is steroid responsiveness. It is important to
toid factor (RF) activity by interacting with IgG IgG4 seems to
make efforts of ruling out malignancy and to take enough biopsy
be associated with a pathogenic effect in a few situations. In pem-
samples. At many institutions, the therapeutic protocol for
phigus, recognition of skin autoantigens (desmogleins) by IgG4 is
IgG4-SC follows that for AIP, such as oral prednisolone with the
at the origin of the disease process In contrast, increased
initial dose of 0.5–0.6/kg body weight/day If lesions do not
inducible-memory Tregs in the periphery and liver tissues are
respond to steroids, re-evaluation to rule out malignancy should
positively correlated with serum levels of IgG4 . In addition,
be performed. In the refractory cases for oral steroids, it has been
prominent infiltration of Tregs upregulated IL-10 in livers of the
reported that steroid mini-pulse therapy , immunomodula-
patients with IgG4-SC . These findings suggest that hyperse-
tors and rituximab are useful.
cretory IgG4 from Tregs may be a secondary phenomenon of thedevelopment of IgG4-SC, whereas overproduction of IgG4 by
Diagnosis of IgG4-SC
BAFF from abnormal innate immunity-related cells such asmonocytes or basophils, may be involved with development of
In many cases of IgG4-SC, diagnosis can be made by a combina-
IgG4-SC. Further studies are necessary to clarify the role of
tion of characteristic biliary images (MRCP, ERCP, and EUS),
IgG4 in IgG4-RD.
increased serum levels of IgG4, coexistence of other organinvolvements (OOIs), and characteristic histopathological fea-
The complement system
tures; however it is sometimes difficult to distinguish from PSC,
Patients in active stages of AIP occasionally show decreased com-
cholangiocarcinoma, and pancreas cancer . Based on these
plement (C3, C4) with elevated circulating immune complex as
findings, the Japanese study group for IgG4-SC proposed the clin-
well as serum levels of IgG4 and the IgG4 subclass of immune
ical diagnostic criteria for IgG4-SC (The effectiveness
complexes. However, a recent study showed that the classical
of steroid therapy is an optional diagnostic criterion to ensure
pathway through IgG1 may be involved in activation of the
accurate diagnosis of IgG4-SC like AIP only after negative workup
complement system rather than mannose-binding lectin or alter-
native pathways through IgG4
Recent advances in the pathogenesis of IgG4-SC
Some patients with IgG4-related disease have non-specific anti-
bodies such as an anti-nuclear antibody (ANA). From the view
Although the precise pathogenic mechanism remains unclear,
of IgG4 function, the big mystery is whether IgG4-related disease
susceptible genetic factors, abnormal innate and acquired immu-
is an autoimmune or an allergic disease. However, the occasional
nity, decreased naïve regulatory T cells, and specific B cell
coexistence of OOIs leads us to consider that there may be
responses may be involved in the development of IgG4-cholangi-
common target antigens in the involved organs, especially the
opathy . The class II antigen haplotype of the human major
pancreas, because of high incidence. Among candidate antigens
Journal of Hepatology 2014 vol. 61 j 690–695

JOURNAL OF HEPATOLOGY
Table 2. The Japanese clinical diagnostic criteria 2012 for IgG4-related sclerosing cholangitis.
1. Biliary tract imaging reveals diffuse or segmental narrowing of the intrahepatic and/or extrahepatic bile duct associated with the
tickening of the bile duct wall
2. Hematological examination shows elevated serum IgG4 concentrations (≥135 mg/dl)
3. Coexistence of autoimmune pancreatiti, IgG4-related dacryoadenitis/sialadenitis, or IgG4-related retroperitoneal fibrosis
4. Histopathological examination shows:
a. Marked lymphocytic and plasmacyte infiltration and fibrosis
b. Infiltration of IgG4-positive plasma cells: >10 IgG4-positive plasma cells/HPF
c. Storiform fibrosis
d. Obliterative phlebitis
Option: effectiveness of steroid therapy
A specialized facility, in which detailed examinations such as endoscopic biliary biopsy and endoscopic ultrasound-guided fine needle aspiration (EUS-FNA) can be administered, may include in its diagnosis the effectiveness of steroid therapy, once pancreatic or biliary cancers have been ruled out
Definite diagnosis
1. + 2. + 4.a., b.
4.a., b., c.
4.a., b., d.
Probable diagnosis
1. + 2. + option
Possible diagnosis
It is necessary to exclude PSC, malignant diseases such as pancreatic or biliary cancers, and secondary sclerosing cholangitis caused by the diseases with obvious pathogenesis. When it is difficult to differentiate from malignant conditions, a patient must not be treated with facile steroid therapy but should be referred to a specialized medical facility.
Modified from Hepatobiliary Pancreat Sci. 2012;19:536–542 Copyright Ó 2012, with permission.
previously reported lactoferrin (LF), carbonic anhydrase
Regulatory T cells
(CA)-II, CA-IV, and pancreatic secretory trypsin inhibitor (PSTI)
Foxp3 is a member of the forkhead/winged-helix family of tran-
are distributed in the pancreas, salivary glands, biliary duct,
scriptional regulators, and functions as the master regulator in
lungs, and renal tubules. Immunization with CA-II or LF induced
the development and function of CD4+CD25+ regulatory T cells
systemic lesions such as pancreatitis, sialadenitis, cholangitis,
(Tregs) classified as naturally occurring CD4+CD25+ Tregs
and interstitial nephritis in the mice models similar to human
(nTregs) originating in the thymus and adaptive Tregs (aTregs)
induced in the periphery by different antigens In IgG4-related diseases, circulatory naïve (CD45RA+) Tregs are signifi-
cantly decreased in the peripheral blood, whereas memory
In addition to steroid and immune-modulators, B cell depletion
(CD45RA�) Tregs are significantly increased In addition,
by rituximab is a useful therapeutic strategy in IgG4-RD. Interest-
prominent infiltration of Tregs with upregulation of IL-10 is
ingly, rituximab reduces only the IgG4 subclass but no other sub-
observed in the liver of IgG4-SC patients These findings sug-
classes of IgG1, IgG2, or IgG3 . A recent study showed
gest that increased memory-Tregs in the periphery and local tis-
expansion of IgG4+ B cell receptor (BCR) clones in blood and tis-
sue of patients with active IgG4-cholangiopathy, and disappear-
inflammation, although decreased naïve Tregs may be patho-
ance by corticosteroid treatment. These findings suggest that
genic. The neonatally thymectomized (nTx)-BALB/c mice with
specific B cell responses may have a pivotal role in the pathogen-
CA-II or LF immunization and WBN/Kob rat models showed
depletion of naïve Tregs and multi-organ inflammation similarto human IgG4-RD These animal models suggested that, in
Th1 and Th2 immune balance
addition to depletion of naïve Tregs, macrophage activation and
The effector cells in IgG4-related diseases have been poorly
Th1 immune responses by CD4+/CD8+ T cells play major roles
understood. The CD4+ T cells differentiate from naïve T cells
in the initial development of organ involvement.
(Th0) to Th1, Th2, Th17, and regulatory T (Treg) cells . In thelivers of IgG4-SC patients, a Th2 type immune reaction is
Our hypothesis for the pathogenesis of IgG4-SC
induced in addition to the Th1 responses Th2 cytokinesmay be involved in the progression of the disease process, espe-
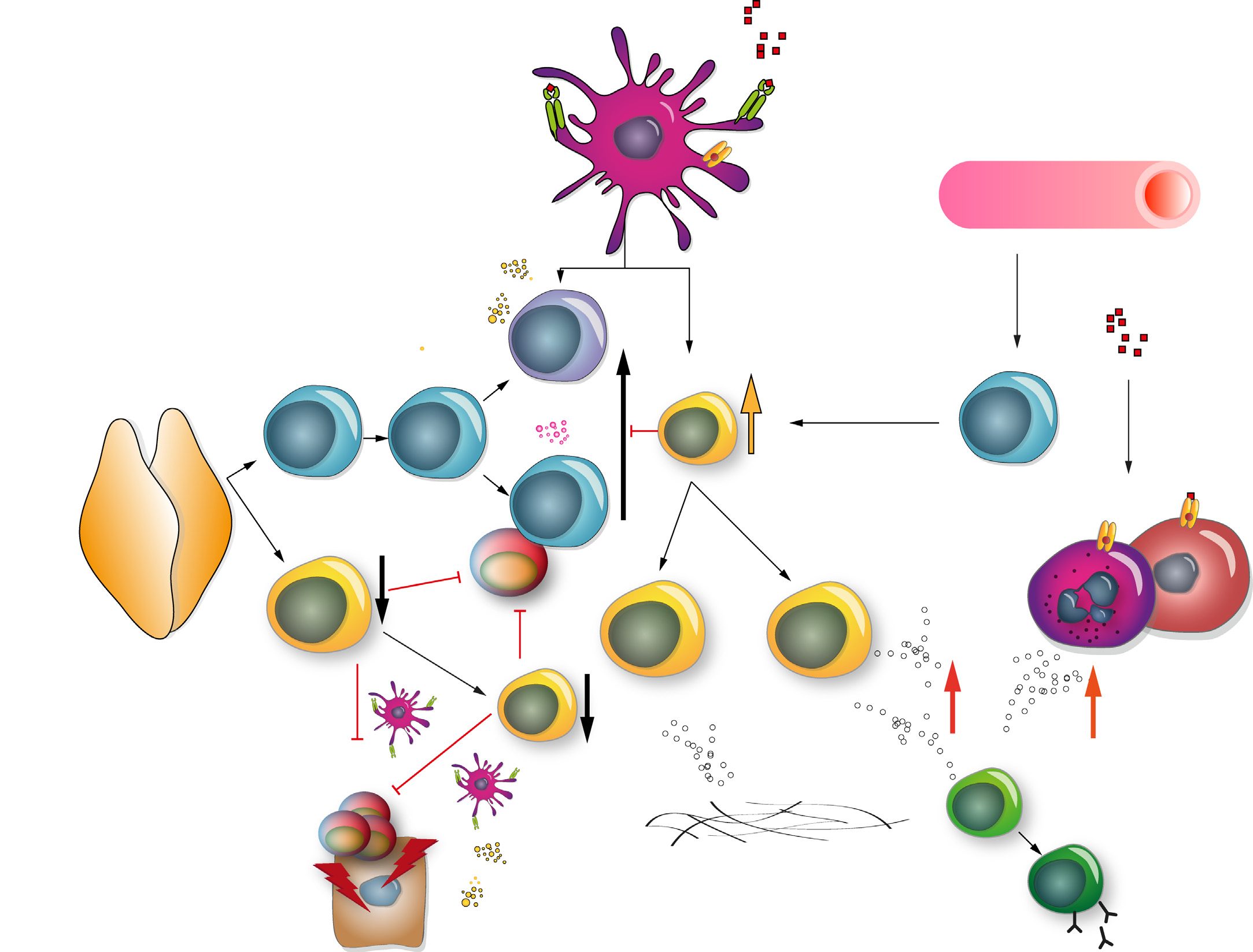
Based on the above findings, we propose the pathogenic mecha-
cially the maturation and proliferation of local B cells and
nisms in IgG4-SC/AIP outlined in . The basic concept is the
biphasic mechanism of ‘‘induction'' and ‘‘progression.'' Initially,
Journal of Hepatology 2014 vol. 61 j 690–695

Clinical Application of Basic Science
Antigens
Hepatology 2007;45:1538
Antigens
Gastroenterology 2000;118:573-581. Pancreas 2006;33:20-26.
J Gastroenterol
Antigens
(LF, CA-II, PSTI,
H. pylori, etc)
Fig. 2. Hypothesis for the pathogenesis of AIP and IgG4-related disease. In the central tolerance, naïve and natural regulatory T cells (Tregs) derived from the thymussuppress autoreactive CD4 or CD8 cells in the normal state. In the IgG4-related disease, the basic concept is the biphasic mechanism of ‘‘induction'' and ‘‘progression''. Initialresponse to antigens (LF, CA-II, CA-IV, PSTI, amylase-alpha, PBP peptide of H. pylori, etc.) might be induced by decreased naïve-Tregs. Th2 immune responses followed byTh1 type immune response with release of proinflammatory cytokines (IFN-c, IL-1B, IL-2, TNF-a). In progression, Th2 type immune responses with producing IgG, IgG4 andautoantibodies may be involved in pathophysiology. IgG4 and fibrosis may be regulated by increased IL-10 and TGF-b secreted from inducible memory-Tregs, respectively.
On the other hand, activation of NOD receptor or TLRs on monocytes or basophils increases IgG4 via upregulation BAFF and IL-13. iTreg, inducible Treg; TE, effector T cell;nTreg, natural Treg; BAFF, B cell activating factor. Modified from J Gastroenterol. 2011;46:277–288 , Copyright Ó 2012, with permission.
decreased naïve-Tregs may induce a Th1 immune response with
Although the pathogenic mechanism remains unclear, we
the release of pro-inflammatory cytokines (IFN-c, IL-1beta, IL-2,
proposed a hypothesis of the pathogenic mechanism of IgG4-
and TNF-a) to unknown antigens such as self-antigens (LF, CA-II,
SC. Further studies are necessary to clarify the pathogenesis
CA-IV, PSTI, and alpha-amylase) or microorganisms (Helicobacter
including genetic backgrounds, disease specific antigens, and
pylori, commensal bacteria, and viruses). Subsequently, Th2 type
the role of IgG4.
immune responses may be involved in the disease progression.
Production of IgG4 may be upregulated by BAFF from monocytesand basophils, and by IL-10 from inducible memory-Tregs. Tumor
Financial support
growth factor (TGF)-beta secreted from inducible memory-Tregsinfiltrating into the involved organ may induce fibrosis.
This study was partially supported by (1) Grant-in-Aid for
Scientific Research (C) of the Ministry of Culture and Science ofJapan (20590810, 24591020, 12008507, 26461038), (2) the
Research Program on Intractable Diseases, from the Ministry ofLabor and Welfare of Japan, and (3) grants-in-aid from the
In conclusion, recent advances support the concept of IgG4-SC, a
Ministry of Education, Culture, Sports, Science and Technology
unique clinical entity as a biliary manifestation of IgG4-RD.
of Japan, from CREST Japan Science, and Technology Agency.
Journal of Hepatology 2014 vol. 61 j 690–695
JOURNAL OF HEPATOLOGY
Conflict of interest
The authors declared that they do not have anything to disclose
regarding funding or conflict of interest with respect to this
Journal of Hepatology 2014 vol. 61 j 690–695
Source: http://demo2.pleksus.com.tr/hpb.org.tr/Uploads/Editor/files/IgG4-kolanjiopatisi-Guncel-kavram-tani-ve-patogenez.pdf
Update on cVEMP and oVEMP testing in Superior Canal Dehiscence Erin Piker, AuD PhD Doug Garrison, AuD • VEMP Background • Recording a VEMP • Clinical Utility of VEMP • Superior Canal Dehiscence • Case Studies Peripheral Vestibular System • 3 semicircular canals (SCC) – Angular acceleration and deceleration • Utricle and saccule – Linear acceleration and deceleration
The Second TSME International Conference on Mechanical Engineering 19-21 October, 2011, Krabi Investigation of Load Profiles of Lithium-ion batteries for Electric Vehicle Applications Chadchai Srisurangkul National Metal and Materials Technology Center, 114 Thailand Science Park, Phahonyothin Rd. Klong 1, Klong Luang, Pathumthani 12120 Thailand







